

Abstract: Pulmonary complications in oesophageal carcinoma are well known and are a major cause of morbidity and mortality. They present as extrinsic compression, airway involvement due to local invasion, and tracheoesophageal fistula (TEF). Tracheal stenting has been effectively used as a treatment to help palliate symptoms and improve the general well-being of the patient. This review focuses on the spectrum of airway involvement in carcinoma of the oesophagus, site of involvement, and the treatment modalities available. The article then focuses on airway stenting and its effect on patients’ symptoms, quality of life, and contribution to overall management while addressing the concerns associated with the stent and its attendant complications.
Key words: Tracheal Stenting, Airway Involvement in Carcinoma Oesophagus, Tracheoesophageal Fistula (TEF).
Introduction
Oesophageal cancer is a major global health challenge, including in India. Worldwide, it is the eighth most common cancer, with an annual incidence of 4.56 lakh new cases. Oesophageal carcinoma is the fourth most common cause of cancer-related deaths in India. Approximately 47 thousand new cases are reported each year in India. A retrospective cohort study from Christian Medical College Hospital, Vellore,1 showed that the majority of cancers affected the upper and middle one-thirds of the oesophagus at the mean age of 51.7 years. Countries with a high human development index (HDI) have a higher incidence of adenocarcinoma, whereas countries with low HDI, such as India, have a higher incidence of squamous cell carcinoma.
Pulmonary Involvement in Carcinoma of the Oesophagus: Review of Literature
Pulmonary complications in carcinoma of the oesophagus are well known and are a major cause of morbidity and mortality. In a study by Cheng et al.2, the main presenting complaints in patients with airway involvement were acute respiratory failure (33.3%), dyspnoea (23.8%), recurrent aspiration pneumonia (19.0%), persistent cough (19.0%), and dysphagia (4.8%). Airway involvement in advanced oesophageal cancer can be in the form of tracheal obstruction, which can be classified as intrinsic or extrinsic. Airway invasion by the tumour may compromise luminal space and produce critical airway narrowing or be extrinsically compressed by the oesophageal growth. Formation of tracheoesophageal fistula (TEF) is also a recognised problem. TEF is an abnormal connection between the trachea and oesophagus seen in approximately 5% to 15% cases. Systemic therapies for the treatment of oesophageal cancer can also predispose to the formation of TEF. Over an 18-year study period, Wang et al.3 found that 26 patients (0.4%) developed airway gastric fistula among 6,316 consecutive patients who underwent oesophagectomy for oesophageal carcinoma. Junyang et al.4, in a retrospective study, found that previous radiotherapy was associated with an increased risk of airway involvement, including Original Articles Review Articles Case Studies The Images Students’ Corner 65 TEF, which had poorer survival compared to TEF attributed to tumour invasion. A common complication of TEF is recurrent non-resolving aspiration pneumonia. Pulmonary sepsis causes fatality in about 6 to 12 weeks if not treated promptly.5,6 Also, these patients are at higher risk of pulmonary embolism and lung atelectasis. Ken Junyang et al.4 retrospectively evaluated data from 804 patients with oesophageal cancer, of which 294 patients were found to have airway involvement. Among patients with airway involvement, 57.1% had airway invasion, 71.4% had compression, and 39.5% had both invasion and compression.
Airway involvement in oesophageal carcinoma can be complex, often involving multiple sites and types of involvement, with the left main bronchus being the most affected site due to its close anatomical relationship with the oesophagus. Nophol et al.5 retrospectively evaluated data of 37 patients who underwent airway stenting for locoregional involvement in patients with carcinoma of the oesophagus. The study showed tumours occurring in the mid oesophagus to be the most common site leading to airway involvement, the upper oesophagus was the second most common location (32.4%) as compared to other sites, followed by upper-middle oesophagus (8.1%), lower oesophagus (5.4%), and upper-middle-lower oesophagus (2.7%). A total of 36.6% of their patients had evidence of airway involvement. The most common site of airway involvement was the left main bronchus (48.6%), followed by the trachea in 12 patients (32.4%). A study by Junyang et al.4 showed a similar trend with midoesophageal tumours being associated with a higher risk of airway involvement. Whereas lower oesophageal cancers rarely affected the central airways.
Airway invasion is the most common involvement at 91.94% and 57.1%, as reported in cohort studies by Cheng et al.2 and Junyang et al.4, respectively. Almost one-third of patients had 70%–90% luminal compression, and 10% patients had critical airway narrowing. Cheng et al.2 reported TEF was present in 14 patients (37.8%), whereas Junyang et al.4 reported it as 35.7%. A 2020 retrospective study from a single gastroenterology centre in India7 evaluated data of the last 20 years and found 7% incidence of TEF. Mixed type of involvement (more than one type) was observed in 78.4% patients.3
A study by Junyang et al.4 found that patients with airway involvement had reduced survival from the time of diagnosis (Hazard ratio: 1.52) and had significantly more hospitalisations per year compared to those without airway involvement. TEF had shorter survival times compared to those with airway involvement but without TEF.
A ray of hope: Airway stenting
Tracheal stenting is a tested and necessary intervention for malignant central airway obstruction and tracheoesophageal fistula. Guidelines by the World Association for Bronchology and Interventional Pulmonology (WABIP) recommend airway stenting in patients with malignant central airway obstruction (MCAO) presenting with attributable symptoms.8
Successful stent deployment has been shown to improve patient's quality of life.9 Another singlecentre study showed that timely airway stenting in MCAO resulted in a significant improvement in Medical Research Council (MRC) dyspnoea scale and Eastern Cooperative Oncology (ECOG) performance scores.10 In a retrospective, single-centre study,11 it was found that in patients with MCAO, a combination of airway stenting and external beam radiotherapy (EBRT) was associated with better survival rates compared to EBRT or stenting alone. Yonghua et al. 12,in a retrospective analysis of combined airway and oesophageal stent implantation for malignant tracheobronchial and oesophageal disease, found that both dyspnoea and dysphagia were significantly relieved, and the survival rates were 82.4%, 78.8% and 78.8% for 1, 3, and 5 years, respectively.
An ideal tracheal stent should be stable and strong to resist the external compressive forces and migration, biocompatible, easily deployed, and removable. The available stent materials include silicone, nitinol, stainless steel, and hybrid stents. Metallic stents made from nitinol and steel are preferred nowadays due to their strength and the ability to exert radial force to keep the airways open. Stents can be self-expandable metallic stents (SEMS) or fixed-diameter stents that may require balloon dilatation. Covered metallic hybrid stents have the advantage that they allow minimal tissue ingrowth and can be easily manipulated. In general, flexible bronchoscopy under local sedation is needed for deployment of these metallic stents.2,3,5
The silicone stents, on the other hand, are versatile and can be easily removed and replaced, which serves a purpose in managing benign airway diseases. They usually require a rigid bronchoscopy and deeper sedation for deployment. The most common silicone stents include Montgomery t-tube, tubular stent, and Y stent.13 Biodegradable stents are under evaluation but are currently not available in India.
The initial concern regarding stents affecting radiation is now being addressed. Early porcine model study by Evans et al.14 showed that metallic airway stents do not significantly affect radiation dose in the airway, and EBRT can be given in a patient with metallic airway stents without affecting the radiation delivered to the tissue.
Airway stenting remains a crucial intervention for patients with malignant airway involvement as it serves as a bridge to further cancer-specific therapy. Many patients who may be rendered non-treatable due to an underlying fragile condition and severe airway complications may improve post-stenting. Nophol et al.5 demonstrated this, where only 48.6% out of 56.7% patients — who received treatment after airway stenting — were found eligible to receive treatment before airway stenting. More patients were eligible to receive concurrent chemoradiation, post-stenting, as it improved their underlying general condition. Patients who received post-stenting treatment had longer survival time (139 days) than those without treatment (57 days). The median survival time after airway stenting was 97 days (interquartile range: 57–199 days). Specifically, airway stenting in treatment-naive patients provided survival benefits, and adjuvant treatment after airway stenting was associated with significantly prolonged survival. The study strongly advocated that airway involvement is not a contraindication for chemoradiation, but airway management should be considered before chemoradiation. The study found that treatment-naive patients and those who received treatment after airway stenting were associated with improved survival. In cases of respiratory failure requiring mechanical ventilation, it may facilitate extubation.
Airway stenting, oesophageal stenting, or both (double stenting) after TEF diagnosis were associated with improved survival. They found that prior radiation was associated with increased risk of airway involvement, increased TEF incidence, and that airway stenting was associated with improved survival.4
A significant issue with airway stenting is the formation of granulation tissue, which can lead to restenosis or airway obstruction.15-17 Stent migration is another complication, particularly in dynamic airway regions, necessitating the regular monitoring of stent positioning.14 Of all the patients that received airway stents, 52.4% had stent-related complications such as mucus plugging (35.7%), tumour ingrowth (38.1%), and granulation tissue formation (7.1%). They found that the incidence of tumour ingrowth was significantly higher in this study (38.1%) when compared to previous data from different studies (5%–24%).
Case 1
We present the case of a 74-year-old female who was evaluated for dysphagia and difficulty in breathing. Upper gastrointestinal (GI) endoscopy showed an eccentric growth at 18 cm–22 cm, and a biopsy confirmed it to be squamous cell carcinoma of the oesophagus. A bronchoscopy was done to evaluate the airways, which showed extrinsic compression of the distal half of the trachea compromising approximately 80% of the tracheal lumen (Figure 1) and tracheal infiltration of the right and left main bronchus. Since the patient had worsening shortness of breath, a SEMS Y stent was placed to cover the lower half of the trachea and both the main stem bronchi (Figures 2 and 3). The patient's general condition improved along with improvement in breathlessness. The patient was started on weekly neoadjuvant chemotherapy (NACT) with injection carboplatin and pacliaqualip. The patient was doing well, with significant improvement in symptom burden after 5 weeks since SEMS insertion.
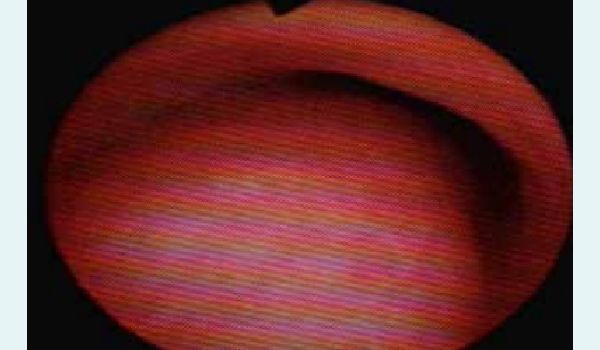
Figure 1: Bronchoscopic examination showing severe tracheal luminal narrowing due to extrinsic compression.

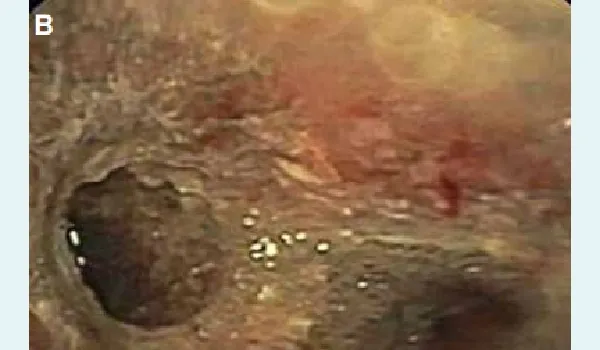
Figure 2(A and B): After the deployment of selfexpandable metallic stent (SEMS) Y stent - Bronchoscopic examination showing near normal lumen of the lower trachea and bilateral mainstem bronchi.
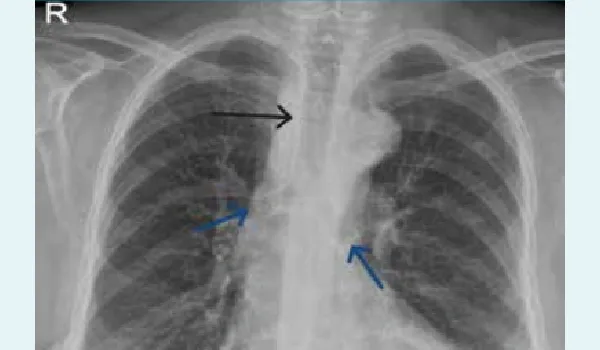
Figure 3: Chest X-ray showing self-expandable metallic stent (SEMS) Y stent placement. Black arrow — Indicates the tracheal limb of the Y stent. This portion is placed within the trachea above the carina; Blue arrow — Points to the right main bronchial limb of the Y stent. This extends into the right main bronchus; Red arrow — Marks the left main bronchial limb of the Y stent. This extends into the left main bronchus.
Case 2
We present a case of a 71-year-old female evaluated for dysphagia, weight loss, and cough while swallowing. Upper GI endoscopy showed an ulceroproliferative growth of 18 cm–27 cm from the upper incisor, completely obstructing the lumen. Biopsy showed well-differentiated squamous cell carcinoma of the oesophagus. Whole body positron emission tomography (PET) and computed tomography (CT) showed metabolically active circumferential wall thickening involving the midoesophagus, approximately 4.7 cm in length. In view of a persistent cough, bronchoscopy was done, which showed a fungating growth involving the posterior and right lateral wall of the lower trachea, causing luminal compromise (Figure 4). A SEMS Y-Stent placement was done (Figure 5). The patient was started on weekly chemotherapy with carboplatin + pacliaqualip. The patient’s general condition improved, and was symptomatically better at 8 weeks after stent and chemotherapy treatment.

Figure 4: Bronchoscopy showing induration with slough in the post wall of the trachea overlying a tracheooesophageal fistula

Figure 5: . Fistula covered with the stent.
Conclusion:
Airway stenting is an active need in patients with airway involvement in cases of advanced oesophageal cancers, which has proven time and again its safety record, amelioration of patient symptoms, improvement in quality of life, and facilitation of further systemic therapy.
Taha Nabeel, Stuti Gupta, Pritha Nayyar, Nikhil Tomar, Ashish Kumar Jain. Tracheal Stenting in Patients
with Malignant Oesophageal Carcinoma: A Comprehensive Review. MMJ. 2025, September. Vol 2 (3).
References
- Samarasam I. Esophageal cancer in India: Current status and future perspectives. Int J Adv Med Health Res. 2017;4(1):5–10.
- Cheng WC, Shen MF, Wu BR, et al. The prognostic predictors of patients with airway involvement due to advanced esophageal cancer after metallic airway stenting using flexible bronchoscopy. J Thorac Dis. 2019;11(9):3929.
- Wang C, Li C, Yang X, et al. The classification and treatment strategies of post-esophagectomy airway-gastric fistula. J Thorac Dis. 2020;12(7):3602.
- Goh KJ, Lee P, Foo AZ, et al. Characteristics and outcomes of airway involvement in esophageal cancer. Ann Thorac Surg. 2021;112(3):912–20.
- Leelayuwatanakul N, Thanthitaweewat V, Wongrishanlai Y, et al. The prognostic predictors of airway stenting in malignant airway involvement from esophageal carcinoma. J Bronchology Interv Pulmonol. 2023;30(3):277–84.
- Shamji FM, Inculet R. Management of malignant tracheoesophageal fistula. Thorac Surg Clin. 2018;28(3):393–402.
- Choksi D, Kolhe KM, Ingle M, et al. Esophageal carcinoma: An epidemiological analysis and study of the time trends over the last 20 years from a single center in India. J Family Med Prim Care. 2020;9(3):1695–9.
- Chaddha U, Agrawal A, Kurman J, et al. World Association for Bronchology and Interventional Pulmonology (WABIP) guidelines on airway stenting for malignant central airway obstruction. Respirology. 2024;29(7):563–73.
- Razi SS, Lebovics RS, Schwartz G, et al. Timely airway stenting improves survival in patients with malignant central airway obstruction. Ann Thorac Surg. 2010;90(4):1088–93.
- Mallow C, Thiboutot J, Semaan R, et al. External beam radiation therapy combined with airway stenting leads to better survival in patients with malignant airway obstruction. Respirology. 2018;23(9):860–5.
- Bi Y, Ren J, Chen H, et al. Combined airway and esophageal stents implantation for malignant tracheobronchial and esophageal disease: A STROBE-compliant article. Medicine. 2019;98(3):e14169.
- Saito Y, Imamura H. Airway stenting. Surg Today. 2005;35(4):265–70.
- Evans AJ, Lee DY, Jain AK, et al. The effect of metallic tracheal stents on radiation dose in the airway and surrounding tissues. J Surg Res. 2014;189(1):1–6.
- Oki M, Saka H, Hori K. Airway stenting in patients requiring intubation due to malignant airway stenosis: a 10-year experience. J Thorac Dis. 2017;9(9):3154.
- Zakaluzny SA, Lane JD, Mair EA. Complications of tracheobronchial airway stents. Otolaryngol Head Neck Surg. 2003;128(4):478–88.
- Burningham AR, Wax MK, Andersen PE, et al. Metallic tracheal stents: complications associated with long-term use in the upper airway. Ann Otol Rhinol Laryngol. 2002;111(4):285–90.
- Jacobs JP, Quintessenza JA, Botero LM, et al. The role of airway stents in the management of pediatric tracheal, carinal, and bronchial disease. Eur J Cardiothorac Surg. 2000;18(5):505–12.