

Abstract: Sexual well-being is integral to overall quality of life; however, diagnosing sexual dysfunction (SD) remains challenging, particularly in India. Diabetes Mellitus (DM), a chronic and progressive condition, is intricately linked to physical, psychological, and sexual health issues, with its comorbidities acting as independent risk factors for SD. This study aimed to assess the prevalence, types, associations, and severity of SD among patients with diabetes.
This cross-sectional study, conducted at Max Superspeciality Hospital in New Delhi, included 340 participants diagnosed with DM. Participants were evaluated using the Arizona Sexual Experience Scale (ASEX), and males were additionally assessed via the International Index of Erectile Function (IIEF)-5. Among participants, 93.8% of males and 53.1% of females were willing to discuss their sexual health. The prevalence of SD was 68.5% in males and 72.5% in females. The most frequently reported SD was dissatisfaction with orgasm, affecting 83% of males and 82% of females. Proteinuria was detected in 94.8% of males and 78% of females. Elevated total cholesterol, low-density lipoprotein cholesterol (LDL-C), and triglycerides were observed, alongside reduced high density lipoprotein cholesterol (HDL-C) levels in males. Notably, 99.3% of males with SD reported erectile dysfunction (ED), with 9.6% experiencing severe ED. SD significantly impacts both genders, with females less inclined to discuss their experiences. Most SD cases involve dissatisfaction with orgasm, and males tend to develop ED and SD earlier in the course of diabetes. Education level, occupation, and smoking status were additional risk factors for SD in males.
Key words: Sexual Dysfunction, Prevalence, Diabetes, Erectile Dysfunction.
Introduction
Kama is a basic instinct, whereas sexual behaviour is learned. Ayurveda identifies Dharma, Artha, Kama, and Moksha as the four Purusharthas — life’s essential goals and fundamental human needs.1 The sexual response cycle, as defined by Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), consists of four phases: desire, excitement (arousal), orgasm, and resolution. It describes the physiological and psychological changes occurring in an individual during sexual arousal and activities such as intercourse and self-stimulation.2 A positive correlation characterises the relationship between an individual's sexual well-being and quality of life.3
Sexual dysfunction (SD) can affect any phase of the sexual response cycle and includes problems with desire (libido), arousal (pelvic vasocongestion causing erections in males and lubrication in females), orgasm (pleasurable rhythmic contractions), and pain during sexual activity. Such pain may prevent individuals or couples from achieving sexual satisfaction. Identifying SD has been particularly challenging in India due to cultural factors. SD causes considerable physical, emotional, and relational distress, significantly impacting the well-being of those affected. Understanding these classifications is essential to addressing this complex and sensitive health issue.4,5
Diabetes mellitus (DM) is a chronic, progressive disorder that can result in various medical, psychological, and SDs. DM is linked to SD in both males and females, with an elevated risk observed at a younger age.5 The prevalence ranges from 20% to 85%.6 Diabetes-related comorbidities such as vascular disease, hypertension, peripheral neuropathy, and obesity independently increase the risk of SD. Individuals with diabetes have a higher prevalence and severity of these conditions compared to the general population. Erectile dysfunction (ED) affects about 36% of diabetic males, nearly three times higher than in non-diabetics. Poor glycaemic control further worsens ED-related morbidity. These factors collectively contribute to the elevated rates and severity of SD in DM.7 Research also shows that individuals diagnosed with diabetes typically develop ED 10 to 15 years earlier than those without the condition.8 The prevalence of ED and premature ejaculation in males correlates with advancing age, hypertension, and diabetes.9
A study conducted by Yaylali et al. demonstrated a higher prevalence of female sexual dysfunction (FSD) in women with DM relative to those without the condition.10 Females with diabetes commonly experience SD, including reduced sexual desire, diminished satisfaction, orgasmic disorder, arousal disorder, and lubrication difficulties.11 Evidence suggests that that the somatic sensory system is altered in diabetes, with the introitus vagina, labium minora, and clitoris identified as the genital regions most adversely impacted. Neuropathy, vascular impairment, and` psychological issues are recognised factors contributing to the development of SD in women with diabetes.12 In addition, endocrine changes can result in diminished vaginal lubrication. Research indicates that female patients with diabetes show a higher incidence of SD than their male counterparts. The presence of diabetes-related complications appears to exacerbate the severity of SD and associated concerns in affected patients.13
The prevalence of ED has been thoroughly examined in male populations because of DM. The phenomenon of SD in females is inadequately addressed in the current literature. SD is acknowledged as a significant health concern that impacts quality of life, significantly affecting both patients and their sexual partners.14 This research has implications for individual health outcomes and societal well-being, enhancing the understanding of patient profiles. ED frequently arises as a common concern in clinical settings. The evaluation of SD in females is often overlooked in clinical assessments. This study sought to assess the prevalence, classifications, and associations of SD in diabetic individuals of both genders, employing internationally recognised assessment instruments.
Methods
Study setting and population
This cross-sectional study was conducted at Max Super Speciality Hospital, Delhi, between February and December 2017. Consenting outpatients aged 18 years and older with a diagnosis of DM and a history of sexual activity within the past year were eligible. Exclusion criteria included a history of pelvic surgery, pre-existing sexual disorders, spouses with sexual diseases, or any significant medical or psychological conditions.
Data collection
A total of 340 patients meeting the inclusion criteria were approached and those providing consent were enrolled. SD was evaluated using the validated Arizona Sexual Experience Scale (ASEX), which assesses libido, arousal, erection or lubrication, orgasm, and satisfaction. An ASEX score > 19 or specific item criteria, indicated dysfunction. All male participants also completed the International Index of Erectile Function (IIEF-5), a validated tool assessing ED severity across five domains, with National Institutes of Health (NIH)-defined cut-off values categorising ED into five severity levels. Both questionnaires are validated tools administered as structured self-reports.
Sample size and statistical analysis
The sample size required to estimate SD prevalence with a 5% margin of error and 80% power was calculated to be 222, consistent with the findings of Marzieh et al. in Iran.14 Statistical analysis was conducted using Statistical Package for the Social Sciences (SPSS) version 16.0. Continuous variables (age, body mass index [BMI], blood pressure, and fasting blood sugar) are presented as mean ± standard deviation, while categorical variables (gender, education, job type), are summarised as percentages. Chi-square tests were used to assess the differences between male and female participants.
Results
A total of 340 patients with DM (210 males and 130 females) were screened over an 11-month period. Of these, 93.8% of males (197 out of 210) and 53.1% of females (69 out of 130) consented to discuss their sexual experiences. Figure 1 illustrates the study flow diagram.
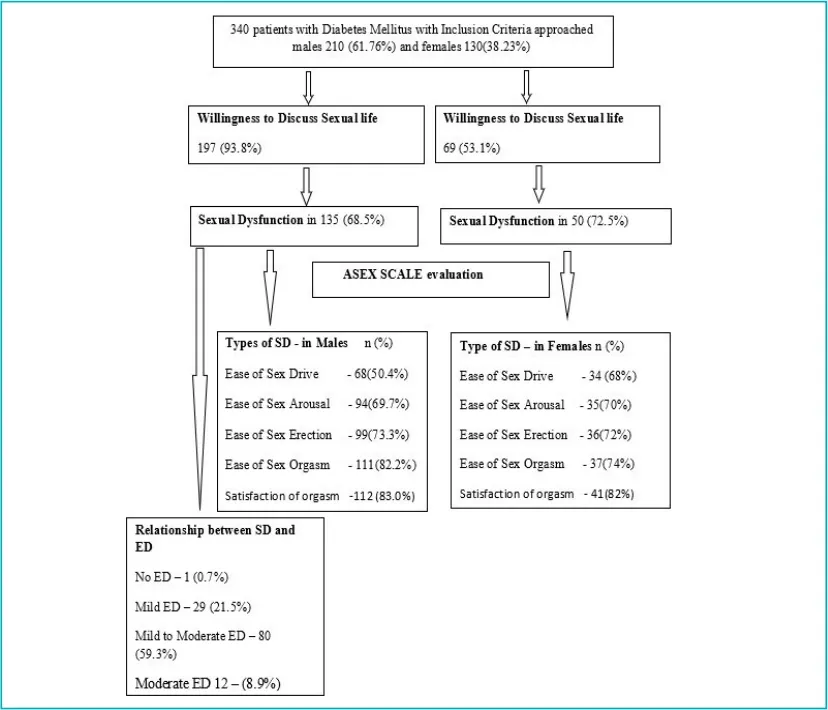
Figure 1: Study flow diagram and demographic characteristics of the study participants.
Abbreviations: ASEX: Arizona Sexual Experience Scale; ED: Erectile Dysfunction; SD: Sexual Dysfunction.
All participants were married, with mean ages of 43.0±7.69 years for males and 43.23±7.80 years for females. Most had type 2 DM (97.1% of males; 99.2% of females), with mean ages at diagnosis of 37.81±7.65 years for males and 39.03±7.71 years for females. Hypertension was present in 51% of males and 45.4% of females, while dyslipidaemia was reported in 49.5% and 45.4%, respectively. The primary method of diabetes management was diet and lifestyle modification (53.3%), followed by oral medications (50.8%). Higher education was achieved by 64.3% of males and 20% of females; 96.7% of males were employed full-time, while 58.5% of females were homemakers. Alcohol consumption (10%) and smoking (4.3%) were reported exclusively among males, and all participants identified as heterosexual.
Prevalence of SD
The prevalence of SD was 68.5% in males (135/197) and 72.5% in females (50/69). Dissatisfaction with orgasm was the most common issue (83% males; 82% females, p = 0.019), followed by difficulty achieving orgasm (82.2% males; 74% females, p = 0.004). (Table 1). Males with SD had a mean age of 42.9 ± 8.0 years (62.2% aged 30–45), while females averaged 46.9 ± 8.1 years (60% aged 46–60). Educational levels differed significantly (p < 0.001): 66.7% of affected males held a college education versus 20% of females. Employment status also varied, with 95.6% of males in full-time employment and 58% females being homemakers.
| Category n (%) | Male n=135 |
Female n=50 |
p-value |
|---|---|---|---|
| Lack of ease in sex drive | 68 (50.4) | 34 (68) | 0.013 |
| Lack of ease of arousal, | 94 (69.7) | 35 (70) | 0.003 |
| Lack of ease of erection, | 99 (73.3) | NA | – |
| Lack of ease of wetness, | NA | 36 (72) | – |
| Lack of ease of orgasm, | 111 (82.2) | 37 (74) | 0.004 |
| Dissatisfaction with orgasm, | 112 (83) | 41 (82) | 0.019 |
Table 1: Types of sexual dysfunction in male and female patients On comparing the metabolic profile, 94.8% of males and 78% of females had proteinuria. Although total cholesterol, LDL-C, and TGs were raised, HDL levels were lower in males as compared to females (p < 0.001) (Table 2).
| Patients with sexual dysfunction | Patients without sexual dysfunction | p-value | |
|---|---|---|---|
| Age | 43.09 ± 7.73 | 43.00 ± 7.70 | < 0.001 |
| Fasting blood sugar (FBS) | 181.28 ± 56.45 | 143.05 ± 9.26 | < 0.001 |
| Glycated haemoglobin (HbA1c) | 8.77 ± 1.99 | 7.64 ± 1.56 | < 0.001 |
| Cholesterol | 241.37 ± 27.27 | 192.54 ± 31.61 | < 0.001 |
| High-density lipoprotein-cholesterol (HDL-C) | 35.78 ± 4.04 | 43.07 ± 4.78 | < 0.001 |
| Low-density lipoprotein-cholesterol (LDL-C) | 114.57 ± 16.47 | 83.40 ± 20.78 | < 0.001 |
| Triglycerides (TG) | 169.08 ± 29.62 | 113.28 ± 42.30 | < 0.001 |
Table 2: Comparison of socio-demographic and clinical variables of patients with and without sexual dysfunction.
Patients with SD had significantly higher FBS, HbA1c, total cholesterol, and LDL-C, but lower triglycerides compared to those without SD (Table 3). Smoking (p = 0.009), hypertension (p = 0.046), and dyslipidemia (p = 0.05) showed significant associations with SD, whereas mean ages did not differ between groups (43.09 ± 7.73 vs. 43.00 ± 7.70).
| Variables | Male n=135 | Female n=50 | p-value |
|---|---|---|---|
| Socio-demographic variables | |||
| Age (years) | 42.89 ± 8.03 | 46.92 ± 8.07 | 0.003 |
| Age group, n (%) | 0.013 | ||
| 30–45 | 84 (62.2%) | 19 (38%) | |
| 46–60 | 49 (36.3%) | 30 (60%) | |
| > 61 | 2 (1.5%) | 1 (2%) | |
| Variables | Male n=135 | Female n=50 | p-value |
|---|---|---|---|
| Socio-demographic variables | |||
| Age (years) | 42.89 ± 8.03 | 46.92 ± 8.07 | 0.003 |
| Age group, n (%) | |||
| 30–45 | 84 (62.2%) | 19 (38%) | 0.013 |
| 46–60 | 49 (36.3%) | 30 (60%) | |
| > 61 | 2 (1.5%) | 1 (2%) | |
| Socio-demographic variables | |||
| Occupation, n (%) | |||
| House maker | 0 (0%) | 29 (58%) | < 0.001 |
| Full-time | 129 (95.6%) | 9 (18%) | |
| Part-time | 5 (3.7%) | 11 (22%) | |
| Unemployed | 0 (0%) | 1 (2%) | |
| Retired | 1 (0.7%) | 0 (0%) | |
| Alcohol, n (%) | 11 (8.1%) | 0 (0%) | 0.037 |
| 124 (91.9%) | 50 (100%) | ||
| Smoking, n (%) | |||
| Current smoker | 2 (1.5%) | 0 (0%) | 0.049 |
| Ex-smoker | 13 (9.6%) | 0 (0%) | |
| Non-smoker | 120 (88.9%) | 50 (100%) | |
| Clinical characteristics | |||
| Type of diabetes mellitus, n (%) | |||
| Type 1 diabetes mellitus | 3 (2.2%) | 1 (2%) | 0.926 |
| Type 2 diabetes mellitus | 132 (97.8%) | 49 (98%) | |
| Age at onset of diabetes (years) | 37.78 ± 7.439 | 42.78 ± 7.939 | < 0.001 |
| Duration of diabetes, n (%) | |||
| 1–5 years | 66 (49.6%) | 29 (58%) | 0.173 |
| 6–10 years | 60 (44.4%) | 21 (42%) | |
| > 10 years | 9 (5.9%) | 0 (0%) | |
| Treatment for diabetes, n (%) | |||
| Diet/lifestyle and oral medications | 77 (57%) | 28 (56%) | 0.899 |
| Injectables (mainly insulin) | 36 (26.7%) | 21 (26%) | 0.927 |
| Injectables (mainly insulin) and oral medications | 22 (16.3%) | 1 (20%) | 0.554 |
| History of hypertension, n (%) | 100 (74.1%) | 13 (26.3%) | 0.793 |
| Dyslipidaemia, n (%) | 73 (54.1%) | 26 (52%) | 0.423 |
| Body mass index (BMI, Kg/m²) | 25.63 ± 1.615 | 25.52 ± 2.002 | 0.702 |
| Systolic blood pressure | 130.37 ± 5.439 | 130.16 ± 6.267 | 0.823 |
| Diastolic blood pressure | 79.75 ± 6.511 | 79.08 ± 6.240 | 0.532 |
| Pulse rate | 90.44 ± 5.914 | 90.02 ± 6.485 | 0.679 |
| Biochemical laboratory parameters, % | |||
| Fasting blood sugar (FBS, mg/dL) | |||
| < 120 | 22 (16.3%) | 15 (30%) | 0.640 |
| > 120 | 113 (83.7%) | 35 (70%) | |
| Glycated haemoglobin (HbA1c) | |||
| 6%–8% | 74 (54.8%) | 29 (58%) | 0.699 |
| > 8% | 61 (45.2%) | 21 (42%) | |
| MAU, mcg/mg of creatinine | |||
| < 30 | 7 (5.2%) | 11 (22%) | 0.001 |
| 30–300 | 128 (94.8%) | 39 (78%) | |
| Total cholesterol | 245.38 ± 22.51 | 230.56 ± 35.26 | 0.001 |
| LDL | 116.54 ± 13.14 | 109 ± 22.538 | 0.007 |
| HDL | 35.04 ± 3.31 | 37.76 ± 5.08 | < 0.001 |
| Triglycerides | 171.64 ± 28.65 | 162.14 ± 31.35 | 0.052 |
| Urea | 14.93 ± 3.22 | 15.50 ± 3.20 | 0.283 |
| Creatinine | 0.78 ± 0.42 | 0.82 ± 0.39 | 0.534 |
Table 3: Socio-demographic factors, clinical characteristics, and laboratory parameters of males and females with sexual dysfunction.
Abbreviations: HDL: High-density cholesterol; LDL: Low-density cholesterol; MAU: Microalbuminuria
Prevalence of ED
Among males with SD, 99.3% (134/135) reported ED. Based on IIEF-5 scores, 9.6% (13/135) had severe ED, while 59.3% (80/135) had mild to moderate ED. Even among males without SD, 81.6% still reported ED, mainly mild (63.2%). The mean age of males reporting ED was 43.05±7.98 years.
Discussion
Female sexual dysfunction (FSD) in India is underresearched, partly due to conservative societal norms and women's traditional roles. While western studies report higher prevalence, Indian research often reports lower rates, likely due to fewer focused studies and the women’s reluctance to discuss sexual health. In this cohort of 340 patients with diabetes, no significant gender difference in SD prevalence was observed, possibly reflecting the unequal gender distribution and female participants' hesitance to discuss sexual experiences. This reluctance may stem from their homemaking role and strong conservative cultural norms in the Indian society.
Among male participants, SD prevalence was 68.5%, slightly higher than the 59.8% reported in Ghanaian men9 and comparable to 63.6% in Chinese diabetic men.10 Female SD prevalence was 72.5%, exceeding the Ghanaian rate of 61.5%9 but lower than the 83% reported by Yaylali et al.10 Other studies show variability, with rates ranging from 51.3% to 71% among women with diabetes.11,12 Such differences across studies may stem from variations in sample selection, SD definitions, assessment tools, and population characteristics such as ethnicity, geography, and diet.
In a 2010 Iranian study, Marzieh Ziaei-Rad et al. reported SD prevalence of 82.5% among diabetic patients, with a significant gender association.14 By contrast, our study reported a 69.5% overall prevalence, with orgasm satisfaction being the most common complaint in both genders (83% in males, 82% in females). Muniyappa et al. noted that diabetes affects desire, arousal, and orgasm, reducing genital sensation and causing vaginal dryness and dyspareunia.13 Our findings align, showing decreased arousal (70%), lubrication (72%), and orgasm (74%) among females with diabetes, underscoring the need to recognise and address FSD in diabetes management.
A vast majority (99.3%) of males with SD reported ED. Notably, 83.6% of males without self-reported SD still exhibited ED, reflecting that while SD is subjective, ED is an objectively measurable condition. SD prevalence was higher in older females compared to males (Table 2). Although many studies suggest SD increases with age, some report no significant age association. Diabetic males show earlier susceptibility to SD and ED, with incidence varying widely (20%–85%),14 often linked to longer diabetes duration. However, several studies report non-significant age correlations with SD, including ED.15
In our study, no significant correlation was found between diabetes duration and either gender or sexual function. SD was more prevalent in both sexes with shorter diabetes duration. Younger males (30–45 years) showed higher SD rates than females, possibly reflecting cultural factors that influence older males’ attitudes toward sexual health. Male sexual function is strongly influenced by psychological and cultural factors, unlike females, who focus more pragmatically on caregiving roles. These findings contrast with some previous research showing a stronger link between diabetes duration and female SD, highlighting inconsistent evidence and the need for further longitudinal studies to clarify this relationship.16,17
Occupation was significantly associated with SD in both sexes. More educated males in managerial or professional roles reported higher SD, possibly due to greater awareness linked to education and occupation, a finding supported by an African study.17 Conversely, most females with SD were less educated homemakers. Additionally, SD prevalence was significantly related to diabetes treatment type, with most affected participants, both male and female, managing diabetes primarily through diet and lifestyle modification.
Our study found that males and females with poor glycaemic control exhibit higher rates of SD compared to those with good control, consistent with findings by Romeo JH et al. High glycaemic levels, which contribute to micro- and macrovascular complications, likely underlie this association.18
Additionally, this study found a significant relationship between lipid abnormalities and SD: males with SD had higher total cholesterol and LDL-C, and lower HDL-C compared with females with SD. Smoking was also gender-related, with male smokers and ex-smokers more prone to SD. Patients rarely discuss SD with healthcare providers, often due to embarrassment or the assumption that providers will address it. Many participants reported negative impacts on relationships, psychological wellbeing, and overall quality of life. Males tended to view SD as a threat to masculinity, whereas females were more accepting of their condition. Poor partner understanding of SD may lead to marital and psychosocial difficulties.
Conclusion:
The research evaluated SD in diabetic patients using validated measures, revealing significant effects in both genders. Females exhibited a lower propensity to engage in discussions regarding sexual issues compared to males. Orgasm dissatisfaction was prevalent in both genders, and most males with SD also reported ED. In males, SD was associated with an earlier onset of diabetes compared to females. The prevalence of SD varied by education, occupation, and employment type, with higher rates observed among more educated, professionally employed males. Lipid profiles also varied by gender, with males exhibiting elevated cholesterol levels and reduced HDL-C levels. Additionally, male smokers exhibited a higher prevalence of SD in comparison to females.
Divya Mangal, Supriya Bali, Sujeet Jha, Vinitaa Jha, Swati Waghdhare, Menka Loomba, Samreen Siddiqui.
Prevalence of Sexual Dysfunction in Men (Erectile Dysfunction) and Women with Diabetes: Types,
Associations, and Severity — An Observational Study from India. MMJ. 2025, September. Vol 2 (3).
References
- Varsakiya J, Kathad D. Facts on male infertility in ancient Ayurveda: historical review. Int Educ Res J. 2018;4(12).
- Shabsigh R, Rowland D. The Diagnostic and Statistical Manual of Mental Disorders, text revision as an appropriate diagnostic for premature ejaculation. J Sex Med. 2007;4(5):1468–78.
- Dogan T, Tugut N, Golbasi Z. The relationship between sexual quality of life, happiness, and satisfaction with life in married Turkish women. Sexuality and Disability. 2013;31(3):239–47.
- Halvorsen JG, Metz ME. Sexual dysfunction, Part I: Classification, etiology, and pathogenesis. J Am Board Fam Pract. 1992;5(1):51–61.
- Mazzilli R, Imbrogno N, Elia J, et al. Sexual dysfunction in diabetic women: prevalence and differences in type 1 and type 2 diabetes mellitus. Diabetes Metab Syndr Obes: Targets Ther. 2015:97–101.
- Maiorino MI, Bellastella G, Esposito K. Diabetes and sexual dysfunction: current perspectives. Diabetes Metab Syndr Obes: Targets Ther. 2014:95–105.
- Abdelhamed A, Hisausse SI, Nada EA, et al. Relation between erectile dysfunction and silent myocardial ischemia in Diabetic patients: A Multidetector Computed tomographic coronary Angiographic study. Sexl Med [Internet]. 2016;4(3):e127–34.
- Siu SC, Lo SK, Wong KW, et al. Prevalence of and risk factors for erectile dysfunction in Hong Kong diabetic patients. Diabetes Med. 2001;18(9):732–8.
- Amidu N, Owired WK, Woode E, et al. Sexual dysfunction among Ghanaian men presenting with various medical conditions. Reprod Biol Endocrinol. 2010;8(1):118.
- Yaylal GF, Tekekoglu S, Akin F. Sexual dysfunction in obese and overweight women. Int J Impot Res. 2010;22(4):220–6.
- Erol BÜ, Tefekli A, Sanli O, et al. Does sexual dysfunction correlate with deterioration of somatic sensory system in diabetic women? Int J Impot Res. 2003;15(3):198–202.
- Doruk H, Akbay E, Cayan S, et al. Effect of diabetes mellitus on female sexual function and risk factors. Arch Androl. 2005;51(1):1–6.
- Muniyappa R, Norton M, Dunn ME, et al. Diabetes and female sexual dysfunction: moving beyond “benign neglect”. Curr Diab Rep. 2005;5(3):230–6.
- Ziaei-Rad M, Vahdaninia M, Montazeri A. Sexual dysfunctions in patients with diabetes: a study from Iran. Reprod Biol Endocrinol. 2010;8(1):50.
- Lewis RW, Fugl-Meyer KS, Corona G, et al. Definitions/epidemiology/risk factors for sexual dysfunction. J Sex Med. 2010;7(4_Part_2):1598–607.
- Ewing DJ. Sexual dysfunction in diabetic men. Pract Diab Int. 1985;2(2):6–9.
- Ungaya GML. The prevalence of sexual dysfunction among patients with diabetes mellitus attending the outpatient diabetic clinic at Kenyatta National Hospital [thesis]. Kuria MW, Owiti FR, editors. University of Nairobi; 2009.
- Romeo JH, Seftel AD, Madhun ZT, et al. Sexual function in men with diabetes type 2: association with glycemic control. J Urol. 2000;163(3):788–91.