

Abstract: Endometriosis affects roughly 10% (190 million) of women and girls of reproductive age globally, having significant social, public health and economic implications. It can decrease quality of life due to severe pain, fatigue, depression, anxiety and infertility. It can present as varied symptoms but presentation as pneumothorax is not only rare but difficult to diagnose. We report a case of a 45-year-old female presenting with recurrent right-sided pneumothorax coinciding with her menstrual cycle. Surgical exploration confirmed the diagnosis. The patient underwent a right-sided video-assisted thoracoscopic surgery (VATS) with repair of diaphragmatic fenestrations and pleurodesis. There was no recurrence of symptoms on follow-up. This case highlights the importance of a high index of suspicion in reproductive-aged women with recurrent pneumothorax. This entity is also termed as catamenial pneumothorax (CP).
Key words: Catamenial Pneumothorax, Thoracic Endometriosis, Diaphragmatic Fenestration, Video-Assisted Thoracoscopic Surgery (VATS), Hormonal Therapy.
Introduction
Catamenial pneumothorax (CP) is one of the manifestations of thoracic endometriosis syndrome (TES), a rare presentation of endometriosis. TES includes catamenial haemothorax, catamenial haemoptysis, and pulmonary nodules predominantly affecting women of reproductive age and usually presenting as rightsided pneumothorax closely associated with the onset of menstruation. The aetiology remains multifactorial, involving retrograde menstruation, prostaglandin-induced bronchospasm, and diaphragmatic fenestrations.1 Given its rarity and often subtle radiologic findings, the diagnosis requires a combination of clinical suspicion, imaging, and intraoperative findings.
Case Report
A 45-year-old female presented with two episodes of sudden-onset right-sided pleuritic chest pain and breathlessness over the past eight months. Both episodes occurred in close association with her menstrual period. No radiological investigations were done at the time of the first episode, and she improved within 2–3 days of conservative management from a local medical practitioner. She denied any history of trauma, smoking, or previous lung disease. During the present episode, she developed sudden and severe shortness of breath, with exacerbation on walking, and was referred to us for further management. Clinical examination during this episode revealed decreased breath sounds in the right hemithorax. Chest radiograph revealed a moderate right-sided pneumothorax (Figure 1). A high-resolution computed tomography (HRCT) scan of the thorax showed no bullous lung disease or parenchymal abnormalities, but confirmed the pneumothorax. Given the recurrent nature and clear association with menses, CP was suspected.

Figure 1: Right-sided pneumothorax with complete collapse of the underlying right lung.
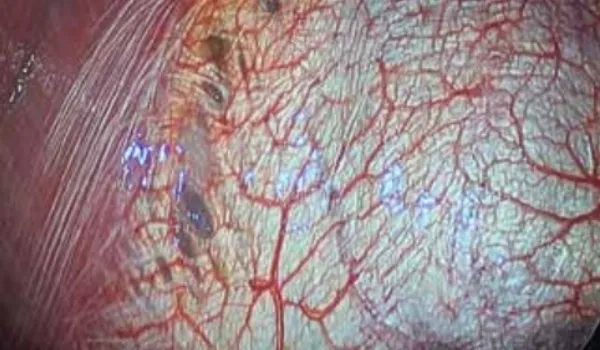
Figure 2: Intra-operative view of diaphragmatic fenestrations with small brownish deposits of endometriosis.
The patient underwent video-assisted thoracoscopic surgery (VATS) under general anaesthesia. Intraoperative findings included multiple small fenestrations in the central tendon of the right diaphragm and brownish deposits on the diaphragmatic surface (Figure 2). The deposits were not large enough for a biopsy. A right-sided VATSguided suture repair of diaphragmatic fenestrations with pleurodesis was performed (Figures 3 and 4).
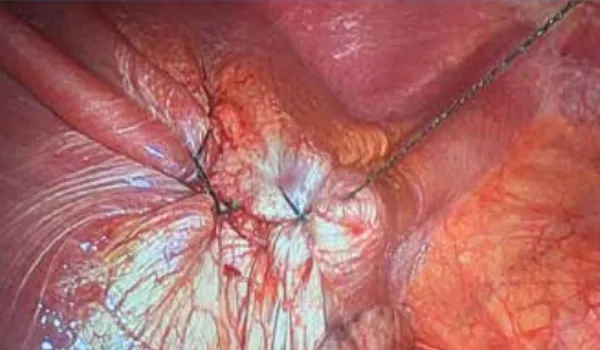
Figure 3: Intra-operative view after diaphragmatic plication of the affected portion of the diaphragm.

Figure 4: Intra-operative view after diaphragmatic plication and talc pleurodesis.
Postoperatively, the patient recovered well and was discharged on the third postoperative day after removal of the chest tube. She is on regular follow-up and prescribed gonadotropin-releasing hormone (GnRH) analogues for 6 months, as per the advice of the gynaecologist.
Review of Literature
CP is a rare but increasingly recognised clinical entity, first described by Maurer et al. in 1958. It is considered the most common manifestation (3%–6%) of TES, which also includes catamenial haemothorax, catamenial haemoptysis, and pulmonary nodules associated with menstrual cycles. CP typically presents as spontaneous pneumothorax occurring within 72 hours of menstruation onset, primarily affecting women of reproductive age, and exhibits a striking right-sided predominance in over 90% of cases.1,2
The pathogenesis of CP is multifactorial and remains incompletely understood. The most widely accepted theories include:
- Transdiaphragmatic migration theory, where endometrial tissue traverses diaphragmatic fenestrations to implant on the pleural surface.
- Microembolisation theory, which suggests haematogenous or lymphatic spread of endometrial tissue to thoracic structures.
- Hormonal hypothesis, where high levels of prostaglandins or hormonal influences lead to vasospasm and alveolar rupture.
- Metaplasia theory, positing that coelomic epithelium differentiates into endometrial tissue under hormonal stimulation.2-4
Surgical findings frequently reveal diaphragmatic defects, fenestrations, and endometrial implants on the pleura or diaphragm. Alifano et al. conducted a pivotal study highlighting that diaphragmatic involvement is present in a majority of surgically treated CP cases, and emphasised the need for thorough inspection of the diaphragm during VATS.1
Joseph and Sahn, in their analysis of 110 cases, provided a framework for the clinical diagnosis of TES, emphasising the importance of menstrual correlation with recurrent pneumothorax.1 Visouli et al. further reinforced the clinical variability of CP in their case series, noting the frequent misdiagnosis and underreporting due to low clinical suspicion.5
Radiologic imaging may be non-specific, with occasional visualisation of diaphragmatic discontinuities or pleural nodules on computed tomography (CT) scans. However, diagnosis is most reliably achieved through thoracoscopic exploration and histopathological confirmation of endometrial glands or stroma, often positive for oestrogen and progesterone receptors.3,6
Management strategies include both surgical and medical approaches. Surgical intervention typically consists of VATS with pleurodesis, pleurectomy, and repair or resection of diaphragmatic lesions, as detailed by Marshall et al. in their treatment algorithm.6 Hormonal suppression using GnRH analogues, progestins, or oral contraceptives helps reduce recurrence by inducing endometrial atrophy.6,7 The recurrence rate following surgery alone is higher compared to combined surgical and hormonal therapy, underscoring the importance of a multidisciplinary approach involving both thoracic surgeons and gynaecologists.5,6
Despite increasing awareness, CP remains an underdiagnosed cause of recurrent pneumothorax. Timely recognition and appropriate combined treatment significantly reduce morbidity and improve long-term outcomes.
Declarations
Patient Consent: Obtained.
Funding: None.
Conflict of Interest: None.
Conclusion
CP, though rare, should be considered in reproductive-age women with recurrent right-sided pneumothorax. Early diagnosis and a combination of surgical and hormonal treatment can effectively prevent recurrence and improve quality of life.
Saraansh Bansal, Pramoj Jindal. Endometriosis Presenting as Pneumothorax: Rare Entity of Thoracic
Endometriosis Syndrome — A Case Report and Review of Literature. MMJ. 2025, September. Vol 2 (3).
References
- Alifano M, Trisolini R, Cancellieri A, et al. Thoracic endometriosis: Current knowledge. Ann Thorac Surg. 2006;81(2):761–9.
- Joseph J, Sahn SA. Thoracic endometriosis syndrome: new observations from an analysis of 110 cases. Am J Med. 1996;100(2):164–70.
- Leong AC, Coonar AS, Lang-Lazdunski L. Catamenial pneumothorax: surgical repair of the diaphragm and hormone treatment. Ann R Coll Surg Engl. 2006;88(6):547– 9.
- Korom S, Canyurt H, Missbach A, et al. Catamenial pneumothorax revisited: clinical approach and systematic review of the literature. J Thorac Cardiovasc Surg. 2004;128(4):502–8.
- Visouli AN, Darwiche K, Mpakas A, et al. Catamenial pneumothorax: a rare entity? Report of 5 cases and review of the literature. J Thorac Dis. 2012;4 Suppl 1(Suppl 1):17–31.
- Marshall MB, Ahmed Z, Kucharczuk JC, et al. Catamenial pneumothorax: optimal hormonal and surgical management. Eur J Cardiothorac Surg. 2005;27(4):662–6.
- Bagan P, Berna P, Assouad J, et al. Value of cancer antigen 125 for diagnosis of pleural endometriosis in females with recurrent pneumothorax. Eur Respir J. 2008;31(1):140–2.