

Abstract:
Chronic obstructive pulmonary disease (COPD) is a progressive respiratory condition that often presents with comorbid mental health disorders, particularly depression, which significantly influences patients' quality of life and disease outcomes. This study aimed to determine the prevalence of depression in COPD patients and identify the associated risk factors while also evaluating their health-related quality of life (HRQoL). A crosssectional observational study was conducted at Max Healthcare's pulmonology outpatient department (OPD). 124 patients aged over 35 years with confirmed COPD and no recent hospitalisations were enrolled. Data were collected using the patient health questionnaire-9 (PHQ-9) to assess depression and the short form-36 (SF36) questionnaire to evaluate HRQoL. Descriptive statistics, logistic regression, and Tukey honest significant difference (HSD) tests were applied to identify significant associations. Depression was prevalent among COPD patients, with significant associations found between higher disability grades and global initiative for chronic obstructive lung disease (GOLD) stages with increased PHQ-9 scores (p = 0.003 and p < 0.001, respectively). Similarly, lower SF-36 scores were significantly correlated with more advanced disease severity (p < 0.001). No statistically significant differences in depression or HRQoL were observed based on gender, age, occupation, education, diet, smoking, or alcohol consumption. Depression is a significant comorbidity in COPD, particularly in patients with severe disease and higher disability grades. Timely psychological assessment and integrated care approaches are essential to improve patient outcomes
Key words: COPD, Depression, PHQ-9, SF-36, Quality of Life, Risk Factors.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic, progressive, and largely preventable lung condition marked by persistent respiratory symptoms and airflow limitation caused by airway and/or alveolar abnormalities. It is primarily due to significant exposure to noxious particles or gases, most commonly tobacco smoke. Globally, COPD poses a major public health challenge and is currently the third leading cause of death, accounting for approximately 3.23 million deaths in 2019 alone.
Although dyspnoea, persistent coughing, and sputum production are the hallmarks of COPD, its effects go well beyond the lungs. A variety of comorbid illnesses are exacerbated by the disease's systemic character, with psychological disorders—especially anxiety and depression being among the most common.2,3 Reduced physical capacity, social isolation, anxiety of dyspnoea, and recurrent exacerbations are some of the factors that contribute to the multifactorial depression associated with COPD.4 In addition to lowering patients' HRQoL, it also makes it harder for patients to follow their treatment plans, which increases the likelihood of hospital stays and raises healthcare expenses.5,6
Depression among individuals with COPD frequently remains underdiagnosed and inadequately treated, despite its common occurrence. While medical professionals may ignore psychological symptoms in favour of treating respiratory conditions, many people mistakenly ascribe mood swings to physical sickness or ageing.7 Additionally, there are gaps in the delivery of care, since conventional COPD management guidelines frequently lack strong foundations for routine mental health screening.8
There appears to be a reciprocal association between depression and COPD. While untreated depression can hinder self-care, reduce medication adherence, and hasten physical deterioration, worsening respiratory function and exacerbations can cause or exacerbate depressive symptoms.9,10 Anxiety and depression frequently combine, with anxiety exacerbating dyspnoea and causing avoidance of activities, which reinforces physical deconditioning.11
Studies have shown that depressive symptoms occur in 10%–60% of COPD patients, depending on disease stage and methodology.12 Additionally, irrespective of lung function, depression is a significant predictor of death.13 Reduced health-related quality of life (HRQoL), elevated symptom burden, and compromised social functioning are all closely linked to these psychiatric comorbidities.14
There is growing agreement that managing COPD requires a multidisciplinary approach that considers both the psychological and physical aspects of the illness. Interventions that have demonstrated encouraging effects in improving outcomes include cognitive behavioural therapy, pulmonary rehabilitation, and pharmaceutical treatment for depression.15 Designing comprehensive care models that promote better quality of life and long-term disease control requires an understanding of the prevalence, severity, and correlates of depression in patients with COPD.
Aim and ObjectivesPrimary objective: To determine the prevalence of depressive symptoms among COPD patients
Secondary Objectives:- To assess the severity of depression in COPD patients.
- To identify demographic, clinical, and lifestyle risk factors associated with depression.
- To evaluate HRQoL using the short form-36 (SF-36) questionnaire.
This cross-sectional observational study was conducted at the pulmonology outpatient department (OPD) of Max Healthcare. Patients over 35 years of age with a confirmed diagnosis of COPD were enrolled after providing informed consent. Participants with recent hospitalisations or known psychiatric illnesses were excluded to minimise confounding factors.
Depression was assessed using the patient health questionnaire-9 (PHQ-9), while HRQoL was measured using the SF-36 questionnaire. Additional demographic and clinical data, such as age, sex, body mass index (BMI), dietary habits, smoking and alcohol history, and disability grades, were recorded. Statistical analysis was performed using the statistical package for the social sciences (SPSS) version 25.0. Descriptive statistics, Pearson’s correlation, logistic regression, and Tukey’s honest significant difference (HSD) tests were used. A p<0.05 was considered statistically significant.
ResultsGender, age, education, occupation, diet, smoking, and alcohol use were among the demographic and lifestyle factors that did not significantly differ in depression (PHQ-9) or quality of life (SF-36) scores, according to the risk factor analysis (p > 0.05) (Table 1). This implies that socio-behavioural factors do not significantly affect depression symptoms and decreased health-related quality of life in individuals with COPD. Figure 1 illustrates the gender distribution among participants, showing a near-equal representation of male and female patients, further supporting the lack of significant association between gender and psychological outcomes. Similarly, figure 2 depicts the age distribution, which demonstrates that depressive symptoms and quality of life scores were not markedly different across age groups. Regardless of their history or lifestyle choices, these findings underscore the necessity of frequent psychological assessment and comprehensive management strategies for all patients with COPD.
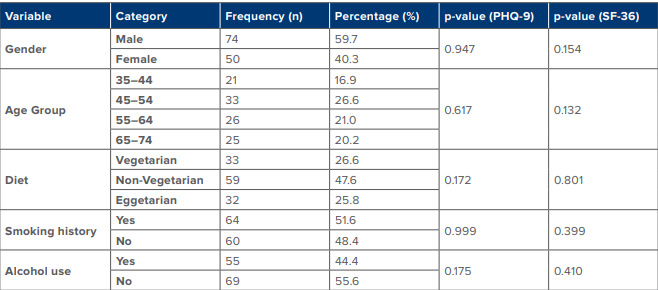
Table 1: Demographics and baseline characteristics.
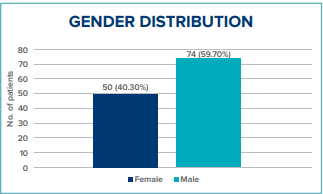
Figure 1: Gender-wise distribution.
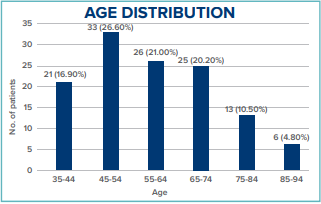
Figure 2: Age group distribution.
Significant associations were observed between disability grades and both depression (PHQ-9) and quality of life (SF-36) scores:
- Grade 5 disability was significantly associated with higher PHQ-9 scores (p = 0.013) and lower SF-36 scores (p = 0.003) (Table 2) and (Figure 3).
- Global (GOLD) stage 4 showed a significantly higher depression score (p < 0.001) and lower HRQoL score (p < 0.001) compared to GOLD stage 1 (Table 3) and (Figure 4).
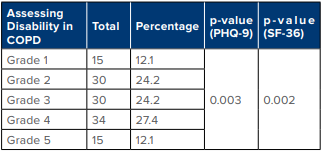
Table 2: Correlation between disability grade and PHQ-9 scores.
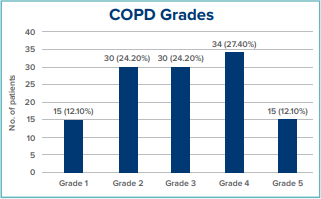
Figure 3: Disability grades in COPD.
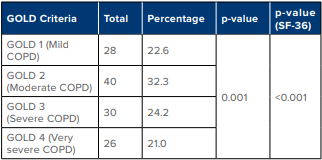
Table 3: GOLD criteria.
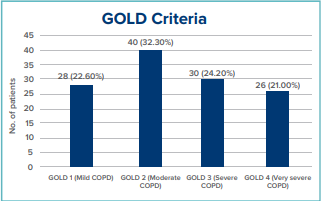
Table 3: GOLD criteria.
A statistically significant inverse association between the severity of depression and health-related quality of life in patients with COPD was found by the correlation analysis using Pearson's coefficient, which showed a substantial negative correlation between PHQ-9 and SF-36 scores (r = -0.807, p<0.001). This indicates that the overall quality of life significantly decreased as depression symptoms rose. The correlation's strength emphasises the significant psychological toll that people with COPD endure and reaffirms how closely mental and physical health are related. These results highlight how crucial it is to detect and treat depression early to potentially enhance the patients' mental health and general quality of life.
Conclusion: This study emphasises the substantial prevalence of depression in individuals with COPD, especially in those with more severe GOLD stages and higher disability grades. The results show a strong relationship between poor respiratory function and a rise in depression symptoms, supporting the idea that patients' physical and mental health significantly deteriorate as the severity of COPD increases.
Discussion
The present study provides compelling evidence of the substantial burden of depression among patients with COPD, a finding that aligns with existing literature. The observed prevalence of depression in our cohort underscores the psychological vulnerability of COPD patients, likely attributable to the chronic nature of the disease, persistent dyspnoea, activity limitation, and social isolation. These factors synergistically diminish patients' quality of life (QoL), further highlighting the bidirectional relationship between COPD and mental health deterioration.
This is consistent with previous research indicating that lower socioeconomic status and unhealthy lifestyle practices exacerbate both physical and psychological morbidity in COPD populations.1,2 Furthermore, the inverse relationship between physical activity and depression severity observed in our study echoes findings from Dogra et al., who emphasised the role of sedentary behaviour in deteriorating mental health among individuals with obstructive lung disease.3
Importantly, our findings also demonstrate a clear link between depression and lower scores on the SF-36, indicating impaired HRQoL. Mental health conditions such as depression can negatively influence COPD self-management, treatment adherence, and engagement in pulmonary rehabilitation, thereby continuing a cycle of poor health outcomes.4 This insight is crucial for clinicians and health policymakers, as it emphasises the need for integrated care models that incorporate routine mental health screening and multidisciplinary interventions for COPD patients.
Although pulmonary rehabilitation has been shown to enhance QoL and reduce depressive symptoms in COPD patients,5 its utilisation remains limited due to accessibility issues and a lack of awareness. Addressing these gaps through targeted public health strategies and patient education may lead to significant improvements in both psychological well-being and functional status.
Conclusion
This study emphasises the substantial prevalence of depression in individuals with COPD, especially in those with more severe GOLD stages and higher disability grades. The results show a strong relationship between poor respiratory function and a rise in depression symptoms, supporting the idea that patients' physical and mental health significantly deteriorate as the severity of COPD increases.
It is interesting to note that the study found no statistically significant correlations between depression and lifestyle or demographic factors, including age, gender, occupation, food, smoking, or alcohol use. This implies that rather than socio-behavioural factors, depression in COPD may be more closely related to the physiological course of the illness. These results highlight how crucial it is to regularly incorporate psychological screening, especially with validated instruments like the PHQ-9, into the clinical evaluation of patients with COPD, irrespective of their behavioural history or background.
Additionally, patients with higher degrees of depression may experience significantly worse HRQoL, as seen by the substantial inverse association between PHQ-9 and SF-36 scores. This emphasises the two-fold burden that people with COPD bear and necessitates a thorough, multidisciplinary management strategy that considers their psychosocial and pulmonary demands. To improve long-term results, early psychological interventions, counselling, and access to mental health services may be essential.
Patients with COPD are very likely to experience depression, particularly if their illness is more advanced and they have more physical limitations. According to the study, depression is more strongly correlated with the severity of the illness than with lifestyle or demographic characteristics. The necessity of routine mental health screening and integrated care that addresses the psychological and physical elements of COPD is further highlighted by a strong negative correlation between depression and quality of life.
Limitations and Future Scope of the StudyThere are various limitations to this study that need to be considered. Determining whether depression causes or contributes to developing COPD is challenging due to the cross-sectional design, which limits causal inferences. Because it was only done at one tertiary care facility, the results might not apply to larger or more varied populations. While the smaller sample size is adequate for preliminary analysis, it may not possess sufficient power to detect variations among smaller subgroups, such as age or occupation. A larger sample size would enhance the robustness of the analysis and improve the ability to identify
these differences. Patients with the greatest psychological burden might have been disregarded since those who had just been admitted to the hospital were not included. Self-reported instruments such as the SF-36 and PHQ-9 add subjectivity and possible reporting bias as well.
To better examine the temporal link between depression and the advancement of COPD, future research should use longitudinal methods. Generalisability would be enhanced by expanding to multicentre studies in a range of socioeconomic and geographic contexts. Biological pathways may become clearer with the use of clinical indicators like oxygen saturation and C-reactive protein (CRP). It is necessary to conduct intervention-based studies to evaluate the effectiveness of pharmacological and psychological interventions in this population. Additionally, incorporating telemedicine and mobile health (mHealth) tools could improve mental health screening and assistance in the treatment of COPD, particularly in settings with low resources or distant locations.
Ayuj Kaushik, Vivek Nangia, Navin Dalal, Ashutosh Yadav.
A Correlation Study to Determine the Prevalence of Depression and Connected Risk Factors Among Patients with Chronic Obstructive Pulmonary Diseases. MMJ. 2025. June. Vol 2 (2).
References
- World Health Organization. Chronic obstructive pulmonary disease (COPD) [Internet]. 2021 [cited 2025 Apr 10]. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
- Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345–349.
- Maurer J, Rebbapragada V, Borson S, et al. Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest. 2008;134(4 Suppl):43S–56S.
- Ng TP, Niti M, Fones C, et al. Co-morbid association of depression and COPD: A population-based study. Respir Med. 2009;103(6):895–901.
- Yohannes AM, Baldwin RC, Connolly MJ. Depression and anxiety in elderly patients with COPD. Age Ageing. 2006;35(5):457–459.
- Cleland JA, Lee AJ, Hall S. Associations of depression and anxiety with gender, age, HRQoL and symptoms in primary care COPD patients. Fam Pract. 2007;24(3):217–223.
- Hill K, Geist R, Goldstein RS, et al. Anxiety and depression in end-stage COPD. Eur Respir J. 2008;31(3):667–677.
- Lopez Varela MV, Montes de Oca M, Halbert RJ, et al. Comorbidities and medication use in patients with COPD. Arch Bronconeumol. 2013;49(9):388–394.
- Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD: A systematic review and meta-analysis. Chest. 2013;144(3):766–777.
- Dalal AA, Shah M, Lunacsek O, et al. Clinical and economic burden of patients diagnosed with COPD with comorbid depression. COPD. 2011;8(4):293–299.
- Di Marco F, Verga M, Reggente M, et al. Anxiety and depression in COPD patients: The roles of gender and disease severity. Respir Med. 2006;100(10):1767–1774.
- van Manen JG, Bindels PJ, Dekker FW, et al. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax. 2002;57(5):412–416.
- Gudmundsson G, Gislason T, Janson C, et al. Depression, anxiety, and health status after hospitalization for COPD. Eur Respir J. 2005;25(3):525–530.
- Eisner MD, Blanc PD, Yelin EH, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65(3):229–234.
- Tselebis A, Pachi A, Ilias I, et al. Strategies to improve anxiety and depression in patients with COPD: A mental health perspective. Neuropsychiatr Dis Treat. 2016;12:297–328.