

Abstract:
Polymyxin B is a potent antibiotic used in multi-drug resistant (MDR) gram-negative infections. It is a known nephrotoxic and neurotoxic drug with serious side effects. Respiratory paralysis is very rarely seen with polymyxin B therapy, with only a few cases reported worldwide. We report a case of a young liver donor who developed respiratory arrest after receiving intravenous (IV) polymyxin B, required intubation, and mechanical ventilatory support. The patient regained full consciousness within an hour. After reviewing literature, we found that polymyxins can cause such side effects. Polymyxin B was discontinued, and she was extubated the following day. With the emergence of MDR organisms, the use of polymyxin B has increased tremendously. This case highlights the importance of closely monitoring patients who are administered such potent antibiotics
Key words: Polymyxin B, Respiratory Arrest, Liver Donor
Introduction
Polymyxin was first isolated in 1947 from the soil bacterium Bacillus polymyxa, which was later reclassified as Paenibacillus polymyxa.1 Polymyxins are small lipopeptide molecules with polycationic peptide ring and a short protruding peptide attached to a fatty acid tail.2 The clinically used polymyxins are polymyxin B and polymyxin E (colistin). They are used for multidrug-resistant (MDR) Gram-negative bacterial infections.3 Their use declined in the 1980s because of nephrotoxicity concerns. However, due to increasing resistance to other antibiotics, the usage of polymyxins has now resurged.4 Polymyxin B is considered less nephrotoxic than colistin and is therefore more commonly used. Respiratory paralysis is an infrequent side effect, with only a few case reports documented globally.5-8
Case report
We report a case involving a 35-year-old female liver donor who underwent a right liver lobe donor hepatectomy. She was previously healthy, with no comorbidities. The intraoperative period was uneventful. In the immediate postoperative period, the patient had an elevated total leucocyte count (TLC) of 20,500/ µL, which progressively increased. We routinely administered cefoperazonesulbactum and amikacin as antimicrobial prophylaxis, which was upgraded to meropenem on day 2. Her liver function tests and liver Doppler ultrasound findings were normal. The patient complained of persistent severe abdominal pain despite adequate analgesia. Pancreatitis was suspected; pancreatic cultures, serum amylase, and lipase were ordered. There was a mild elevation of amylase and lipase consistent with pancreatitis. The patient’s TLC increased further to 37,000/ µL on day 4, along with fever spikes (Table 1). Given the recent occurrence of multiple MDR infections in the intensive care unit (ICU) and concerns for donor safety, the patient was started on polymyxin B. One hour after a loading dose of 15 lakh units infused over 1 hour, the donor complained of breathing difficulty and became apnoeic almost immediately. She was intubated and placed on mechanical ventilator support. The patient regained full consciousness within an hour of the event and responded well with minimal pressure support on the ventilator. After ruling out administration errors or unintended medications, her drug chart was carefully reviewed. Literature review confirmed that polymyxin B is associated with rare but serious adverse effects, including respiratory arrest, especially when combined with aminoglycosides. Our patient had been receiving amikacin until the day prior. polymyxin B was discontinued, meropenem was continued, and the patient was electively ventilated overnight. The patient was extubated the following day. All cultures were reported negative, her TLC gradually decreased, and she was discharged home on day 10.
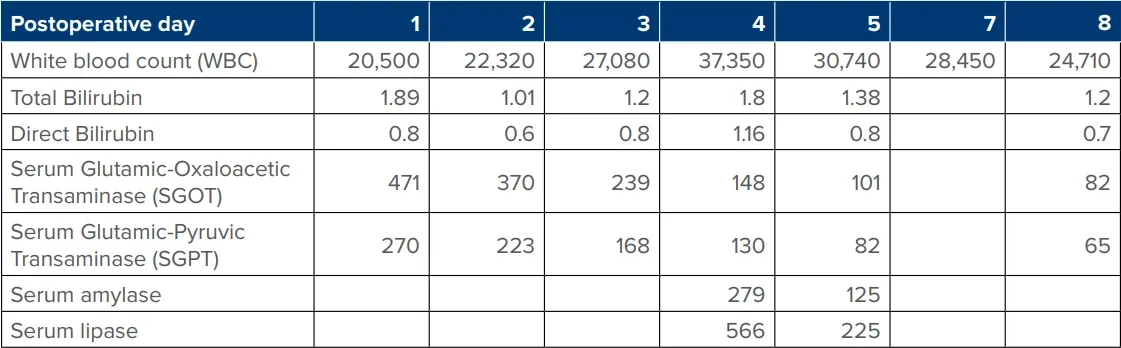
Table: Postoperative laboratory trends.
Discussion
Although now widely used, polymyxin B is associated with serious side effects, including nephrotoxicity and neurotoxicity. The incidence of nephrotoxicity ranges from 20%-60%, and neurotoxicity occurs in approximately 7% of cases.4
Respiratory paralysis is a rare but potentially lifethreatening side effect with only a few case reports. In 1968, Lindesmith et al. first reported 11 cases of polymyxin-induced respiratory paralysis.9 Neuromuscular blockade may occur at both pre- and post-synaptic sites. Presynaptic dysfunction occurs due to non-competitive blockade, which results in reduced acetylcholine release into the synapse.9 Other mechanisms include calcium depletion and prolonged depolarisation.10 This blockade is not reversed by cholinesterase inhibitors. The onset of paralysis may range from 1 to 26 hours following polymyxin B administration. Risk factors for this adverse effect include renal failure, concurrent use of nephrotoxic medications, certain antibiotics (particularly aminoglycosides), higher doses of polymyxin B, and female gender.11,12
Most reported cases involve elderly and sick individuals with some renal dysfunction.5-7,9
However, our patient was a young, healthy donor with normal renal function. With the increase in home-care nursing facilities, potent antibiotics are routinely given at home. This case highlights the need to administer such potent antibiotics cautiously.
Conclusion
Although respiratory paralysis is a rare adverse effect of polymyxin B therapy, clinician awareness of such side effects is essential. With the increasing prevalence of MDR infections, the use of higher-end antibiotics has risen significantly, heightening the risk of such rare but serious events. This case underlines the importance of cautious use and close monitoring of such agents, even in otherwise healthy individuals.
D Navakanth, Sunita Verma, Vachaspati Kumar, Kshitij Sisodia, KR Vasudevan. Polymyxin B
Therapy-Induced Respiratory Arrest in a Liver Donor: A Case Report. MMJ. 2025, June. Vol 2 (2).
References
- Storm DR, Rosenthal KS, Swanson PE. Polymyxin and related peptide antibiotics. Annu Rev Biochem. 1977;46:723-763.
- Nation RL, Velkov T, Li J. Colistin and polymyxin B: Peas in a pod, or chalk and cheese? Clin Infect Dis. 2014;59: 88-94.
- Nation RL, Li J, Cars O, et al. Framework for optimisation of the clinical use of colistin and polymyxin B: The Prato polymyxin consensus. Lancet Infect Dis. 2015;15:225-234.
- Landman D, Georgescu C, Martin DA, et al. Polymyxins revisited. Clin Microbiol Rev. 2008;21:449-465.
- Wunsch H, Moitra VK, Patel M, et al. Polymyxin use associated with respiratory arrest. Chest. 2012;141(2):515-517.
- Ramasubban S, Sen S, Kumar M S, et al. Polymyxin B infusion related respiratory arrest: A case report. IP Indian J Immunol Respir Med. 2021;6(4):241-244.
- Ning Y, Chu Y, Wu Y, et al. Case Report: Respiratory paralysis associated with polymyxin B therapy. Front Pharmacol. 2022;13:963140.
- Chen WH, Lin L, Wang XX, et al. Respiratory arrest associated with polymyxin B in a lung transplant patient. Chinese medical journal. 2020;133(11):1375-1377.
- Lindesmith L A, Baines RD, Bigelow DB, et al. Reversible respiratory paralysis associated with polymyxin therapy. Ann. Intern. Med. 1968;68(2):318-327.
- Kubikowski P, Szreniawski Z. The mechanism of the neuromuscular blockade by antibiotics. Arch Int Pharmacodyn Ther. 1963;146:549-60.
- Falagas ME, Kasiakou SK. Toxicity of polymyxins: a systematic review of the evidence from old and recent studies. Crit Care. 2006;10(1):R27.
- Sokoll MD, Gergis SD. Antibiotics and neuromuscular function. Anesthesiology. 1981;55(2):148-159.