

Abstract:
Robotic surgery has recently evolved and is rapidly augmenting both endoscopic and conventional open surgeries. Robotic surgery is currently used for thyroid surgeries for both benign and malignant conditions offering less invasive surgical options, better cosmesis, faster recovery, and reduced morbidity. Its use has also been reported in congenital conditions presenting as neck swellings, such as thyroglossal cysts, branchial cysts, and cystic hygromas. Robotic surgery provides excellent visualisation and ergonomically favourable access to deep-seated neck masses, while preserving aesthetic integrity by avoiding open cervical incisions. With careful patient selection and appropriate surgical expertise, it ensures a safe, effective, and cosmetically superior alternative to traditional open surgery.
Key words: Neck Masses, Thyroid, Branchial Cleft Cyst, Thyroglossal Cyst.
Introduction
CCongenital neck masses are present at birth and can result from developmental anomalies such as branchial cleft cysts, thyroglossal duct cysts, and cystic hygromas. These masses typically present in childhood but can persist into adulthood if left untreated. Other congenital causes include dermoid cysts, teratomas, and vascular anomalies like haemangiomas and lymphangiomas.
Branchial cleft anomalies form due to incomplete involution of branchial cleft structures. Around the fourth week of gestation, neural crest cells migrate into the future head and neck region, where six pairs of branchial arches begin to develop. The mesoderm is covered externally by ectoderm and internally by endoderm. Although there are six pharyngeal arches, in humans, the fifth pharyngeal arch exists only transiently during embryogenesis.
The five pharyngeal arches are separated by depressions known as clefts on the ectodermal surface, and corresponding pouches on the endodermal surface, yielding four pharyngeal clefts. The ventral part of the first cleft obliterates, whereas the dorsal part gives rise to the external acoustic meatus and pinna. Normally, the second to the fourth clefts obliterate due to overgrowth of the second pharyngeal arch.1
Branchial cleft cysts are the second most common congenital anomalies of the head and neck, following thyroglossal duct anomalies.2 They result from the incomplete fusion of a pharyngeal cleft.
The second pharyngeal cleft is the source of the most prevalent type of branchial cyst; abnormalities originating from the first, third, and fourth clefts are less common.3
Congenital anomalies exist from birth, even if they might not be noticeable or symptomatic right away. Most lesions manifest as a cutaneous punctum in childhood, although they can also appear as cysts or neck lumps.4,5 Anomalies involving branchial cysts can manifest as cysts, sinuses, or fistulae.6,7
According to the Bailey-Proctor classification (Figure 1),8 second branchial cysts are divided into four types:
- Type-I cysts are located along the anterior border of the sternocleidomastoid muscle, beneath the superficial cervical fascia.9,10
- Type-II cysts are the most common and are located just laterally to great vessels beneath enveloping fascia of the neck.11,12
- Type-III cysts pass between the internal and external carotid arteries.
- Type-IV cysts are located in the pharyngeal mucosal space, just deep to the palatine tonsil and medial to great neck vessels, often extending upward towards the skull base.13,14
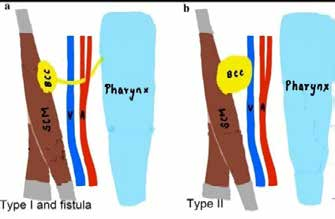
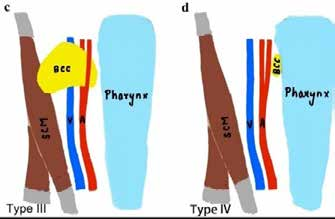
Figure 1: Bailey Proctor Classification
Case Report
A 29-year-old female presented to the OPD with a chief complaint of swelling in the left submandibular region for the last six months and pain in the swelling for the last three days, associated with high-grade fever. There was no history of trauma or any other event that could be suspected of contributing to the onset of the swelling. The patient denied history of dysphagia, dyspnoea, dysphonia, or any other symptoms of nerve involvement. The swelling was initially small in size and gradually progressed to its current size. It was not associated with any pain until the last three days.
On clinical examination, a solitary swelling measuring 10 cm x 8 cm was noted in the left submandibular region (Figure 2), extending from the angle of the mandible posteriorly (not crossing the sternocleidomastoid muscle) till the submental region anteriorly, crossing the midline, with superior extension to the mesenteric region. There was associated erythema of the overlying skin. The pinchable overlying skin was warm and tender to palpation, with a soft consistency. The swelling was immobile in either direction. There was no limitation in mouth opening.

Figure 2: Showing a large swelling in the submandibular region (Preoperative)
The patient was admitted to the surgical ward for further evaluation. Baseline investigations revealed leucocytosis (total leucocyte count: 14,000/ mm3 ), while the rest of the routine laboratory investigations within normal limits. To better delineate the extent of the swelling, an magnetic resonance imaging (MRI) of the neck was performed, which revealed a large well defined, smooth walled septate cystic lesion in the left submandibular region, located below the level of the mylohyoid muscle. The lesion was bulging superomedially, medial to the mandibular body and extended laterally to reach the skin surface, with associated dilatation of the Wharton's duct (Figure 3).


Figure 3: T2-weighted magnetic resonance imaging (MRI) images (A) coronal view (B) sagittal view of head and neck region .
To further assess the vascular involvement, a computed tomography (CT) angiography was performed, which revealed splaying of the branches of the external carotid artery by the swelling. (Figure 4)
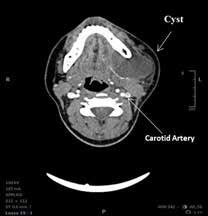
Figure 4: Computed tomography (CT) angiography of neck showing cyst in close approximation with the submandibular gland and carotid artery in retro-mandibular space.
Based on clinico-radiological correlation, a diagnosis of Type II branchial cleft cyst was made. The patient expressed cosmetic concerns regarding a visible surgical scar, and as a consequence, robotic excision of the branchial cyst was planned. Three ports were created (Figure 5): 8mm circum-areolar port, a 5 mm upper axillary port, and an 8 mm endoscope port in the anterior axillary line. An endoscope was introduced and a dissection plane was created. A robotic dock was then used to allow for improved manoeuvrability in the deep and narrow surgical space. Finally, the cyst was excised along with the submandibular gland, with preservation of the lingual and facial nerves, and careful dissection away from the carotid artery (Figure 6).

Figure 5: Showing the port sites for excision.
Figure 6: Separation of branchial cyst wall adherent to the submandibular gland.
The specimen was completely excised and sent for histopathological examination. The findings were consistent with a lymphoepithelial cyst. The postoperative course was uneventful. The patient was discharged on postoperative day (POD) 2. The patient was reviewed on POD 5, when a significant reduction in the swelling was noted. (Figure 7).

Figure 7: Postoperative follow up image
Discussion
Type II branchial cleft cysts are the most prevalent congenital anomalies making up to 90%-95% of branchial cleft cysts. They are typically asymptomatic in infancy and childhood but can become symptomatic later in life due to infection or trauma. In this case, a female patient presented with pain and swelling in the left submandibular region, along with high-grade fever. The diagnosis remained broad until the patient was admitted for detailed evaluation.
Radiological investigations play a key role in differentiating congenital neck masses.12,13 In this case, an MRI revealed a well-defined, large, smooth- walled septate cystic lesion, a classic feature of a Type II branchial cleft cyst. The cyst was located lateral to the great vessels and beneath the mylohyoid muscle, confirming the diagnosis of a branchial cyst.
A CT angiography was also done to confirm the diagnosis and assess if there was any vessel involvement. The CT angiography confirmed that the external carotid artery was not encased by the cyst, supporting a robotic excision approach. The robotic technique was chosen due to its precision in an extremely sensitive anatomical region, aiming to avoid complications. Its binocular 3D high-definition vision and precise ergonomic movements enables surgeons to perform complex surgeries in deep and narrow areas with better precision.
Despite the cyst’s large size (approximately 10 × 8 cm), robotic excision allowed for complete removal and safe dissection from the surrounding vascular structures and the submandibular gland. This was achieved without complications and with minimal scarring, a significant advantage over traditional open surgery. The patient benefited from improved cosmetic outcomes.
Ethical Approval
This case report has been reported in line with the Surgical CAse REport (SCARE) criteria.
Sources of Funding
None
Conflict of Interest Disclosure
The authors declare that they have no financial conflicts of interest in relation to the content of this report.
Conclusion
- Recent advances in minimal invasive surgery, particularly using robotic techniques, are gaining popularity. The scope of robotic surgery continues to expand rapidly. This case report highlights the importance of imaging for an accurate diagnosis and the clinical and cosmetic advantages of robotic excision of a branchial cleft cyst.
Vikas Panwar, DV Sneha, Sourav Panda. Robotic Surgery for Congenital Branchial Cleft Cyst Presenting in Young Adults. MMJ. 2025, June. Vol 2 (2).
References
- Coste AH, Lofgren DH, Shermetaro C. Branchial Cleft Cyst. [Updated 2023 Jun 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearlsPublishing; 2025 Jan.
- Patel S, Bhatt AA. Thyroglossal duct pathology and mimics. Insights Imaging. 2019;10(1):12.
- Bahakim A, Francois M, Van Den Abbeele T. Congenital Midline Cervical Cleft and W-Plasty: Our Experience. Int J Otolaryngol. 2018;2018(1):5081540.
- Banakis Hartl RM, Said S, Mann SE. Bilateral Ear Canal Cholesteatoma with Underlying Type I First Branchial Cleft Anomalies. Ann Otol Rhinol Laryngol. 2019;128(4):360-364.
- Meng F, Zhu Z, Ord RA, Zhang T. A unique location of branchial cleft cyst: case report and review of the literature. Int J Oral Maxillofac Surg. 2019;48(6):712-715.
- Prosser JD, Myer CM. Branchial cleft anomalies and thymic cysts. Otolaryngol Clin North Am. 2015;48(1):1-14.
- Magdy EA, Fadali GA, Seif-Elnasr M, et al. Unusual Isolated Parapharyngeal Second Branchial Cleft Cyst: A Case Report and Literature Review. Case Rep Otolaryngol. 2020;8814071.
- Work WP. Newer concepts of first branchial cleft defects. Laryngoscope. 1972;82(9):1581-93.
- Bajaj Y, Ifeacho S, Tweedie D, et al. Branchial anomalies in children. Int J Pediatr Otorhinolaryngol. 2011;75(8):1020-3.
- Muller S, Aiken A, Magliocca K, et al. Second Branchial Cleft Cyst. Head Neck Pathol. 2015;9(3):379-83.
- Nicoucar K, Giger R, Pope HG, et al. Management of congenital fourth branchial arch anomalies: a review and analysis of published cases. J Pediatr Surg. 2009;44(7):1432-9.
- Brown RE, Harave S. Diagnostic imaging of benign and malignant neck masses in children-a pictorial review. Quant Imaging Med Surg. 2016;6(5):591-604.
- Prada LR, Koripalli VS, Merino CL, et al. A Case of a Rapidly Enlarging Neck Mass with Airway Compromise. J Clin Diagn Res. 2017;11(5):OD14-OD16.