

Abstract:
Ganglioneuromas are rare, benign tumours arising from sympathetic neural crest cells, often detected incidentally or when large enough to cause compressive symptoms. Their proximity to critical retroperitoneal vascular structures can complicate management.
A 28-year-old female presented with progressive abdominal pain, fullness, and backache. Imaging revealed a large retroperitoneal lobulated lesion around the coeliac axis extending into the right suprarenal region, encasing the hepatic artery. Biopsy confirmed a ganglioneuroma. After being denied surgery initially due to operative risks, she underwent successful surgical excision at a tertiary centre. The mass was dissected from major vessels, including the hepatic artery, coeliac axis, portal vein, pancreas, and inferior vena cava via a midline incision with full Kocherisation.
Complete resection of retroperitoneal ganglioneuroma, though surgically challenging due to vascular encasement, is feasible and curative with meticulous dissection and multidisciplinary expertise.
Key words: Ganglioneuroma, Sympathetic Neural Crest Cells, Retroperitoneal.
Introduction
Ganglioneuromas are benign, differentiated tumours arising from sympathetic ganglion cells and Schwann cells. Representing the benign end of the neuroblastic tumour spectrum, they are most commonly located in the posterior mediastinum and retroperitoneum. Due to their slow growth, symptoms typically present late when the mass becomes sizable or causes compression of adjacent structures.
Surgical excision remains the gold standard for treatment. However, involvement of major vascular structures such as the hepatic artery, portal vein, or inferior vena cava can increase surgical complexity and risk.1
This report describes a case of a large retroperitoneal ganglioneuroma encasing the hepatic artery in a young adult female, managed successfully through complex surgery.
Case Report
A 28-year-old female presented to a government hospital with a six-month history of progressive abdominal pain, upper abdominal fullness, and dull backache. She had no significant medical history or systemic complaints. Physical examination was unremarkable apart from upper abdominal tenderness. Routine laboratory parameters were within normal limits. Computed tomography (CT) scan of the abdomen revealed a large, lobulated lesion measuring 116 x 53 x 97 mm with enhancing septations and calcific foci, situated in the right suprarenal region. The lesion encased the hepatic artery anteriorly and displaced adjacent vascular and visceral structures, including the coeliac axis, portal vein, pancreas, and inferior vena cava (Figure 1).
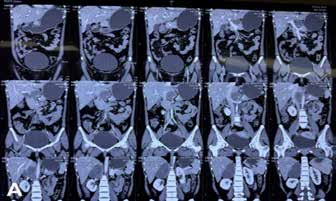
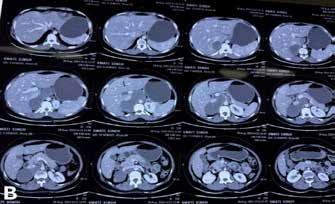
Figure 1: Contrast-enhanced computed tomography (CT) images showing a large lobulated retroperitoneal mass encasing the hepatic artery and displacing adjacent structures. (A) Coronal plane. (B) Axial plane.
An image-guided core needle biopsy was performed, and histopathology revealed mature ganglion cells within a Schwannian stroma, confirming the diagnosis of ganglioneuroma.
Due to extensive vascular involvement and the risk of intraoperative haemorrhage, the patient was denied surgical treatment at the initial government facility.
Seeking further management, she presented to Max Super Specialty Hospital, Lucknow, where a multidisciplinary tumour board recommended surgical excision.
Surgical Procedure
A midline laparotomy with full Kocherisation was performed. Intraoperatively, the mass was found arising near the coeliac axis, extending laterally below the pancreas and portal vein, and reaching below the inferior vena cava. It was noted to encase the hepatic artery anteriorly (Figure 2A).

Figure 2A: Intraoperative image showing the lobulated retroperitoneal mass.
Key surgical steps followed were:-
Dissection of the portal structures and hepatic artery up to the coeliac axis.
-
Mobilisation between the mass and superior border of the pancreas and the superior mesenteric artery
-
Dissection of the mass away from the lesser sac and retro-pancreatic space.
-
Mobilisation of the remaining mass from the inferior vena cava.
The surgery lasted four hours with an estimated blood loss of 150 mL.
Histopathology
Gross examination of the excised specimen showed a lobulated, firm, grey-white mass (Figure 2B).

Figure 2B: Resected lobulated, grey, firm mass.
Microscopic examination revealed well-circumscribed tumour tissue composed of an admixture of predominantly Schwann cells and scattered ganglion cells. Schwann cells displayed spindle-shaped morphology with elongated, bland nuclei and loose, fibrillary, homogenous, eosinophilic cytoplasm. Ganglion cells, on the other hand, were mature, exhibiting a single eccentric round nucleus, a prominent nucleolus, and compact, granular, eosinophilic cytoplasm, with some showing occasional pigment deposition. No naked neuropil, neuroblastic foci, atypia, or mitoses were present (Figure 3). A final diagnosis of ganglioneuroma, maturing (Schwannian stroma predominant) was established.
The patient had an uneventful postoperative recovery and was discharged on the ninth postoperative day.
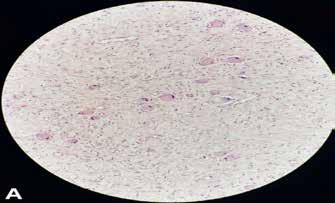
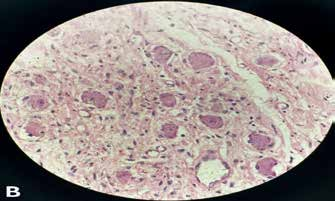
Figure 3: Mature ganglion cells and Schwannian stroma consistent with ganglioneuroma. (A) Tissue section (H & E x20). (B) Tissue section (H & E x40).
Discussion
Neuroblastic tumours (NTs) are the most common solid neoplasm of childhood, arising from primordial neural crest cells located in the sympathetic ganglia and adrenal medulla. The vast majority of them are sporadic. NTs are divided into three categories: Neuroblastoma, ganglioneuroblastoma, and ganglioneuromas (GN). GNs typically present in the fourth or fifth decade of life. They are most commonly found in the retroperitoneal space (32%-52%) and the posterior mediastinum (39%-43%), with less frequent occurrences in the cervical region (8%-9%).2 Unlike other neuroblastic tumours, GNs are generally hormonally silent and are often diagnosed incidentally on radiography, or present as a large mass with symptoms of compression.3,4 According to the International Neuroblastoma Pathology Classification (INPC), GNs are subtyped into GN, maturing and GN, mature.5 The GN, maturing subtype was formerly classified as “stroma-rich, well-differentiated NT” in the original Shimada classification. GN, mature subtype is the prototypic GN of traditional classification schemes. Less than 30% of these tumours occur in the adrenal glands and are usually asymptomatic. The remainder develops in the posterior compartment of the mediastinum, retroperitoneum, and other sites. Rarely, they can be associated with hypertension, watery diarrhoea, and hypokalaemia or masculinisation.6
CT and magnetic resonance imaging (MRI) play pivotal roles in preoperative assessment, delineating the extent of vascular involvement, which critically influences surgical planning. Characteristically, these tumours appear as well-defined, lobulated masses with homogeneous or heterogeneous enhancement and may contain calcifications.4,7
Histopathological confirmation is mandatory, with biopsy demonstrating mature ganglion cells within a Schwannian stroma and absence of immature neuroblastic elements.1,5,8
Surgical excision remains the cornerstone of treatment. Cases involving major vascular encasement require advanced surgical expertise and careful intraoperative dissection to prevent catastrophic bleeding and preserve vital vascular anatomy.
This case underscores the feasibility of complete excision even in complex presentations with vascular involvement, highlighting the role of multidisciplinary care in achieving optimal outcomes.
Chakradhar Singh, Shashank Chaudhary, Anju Shukla. Unmasking a Silent Giant: Complicated Resection of a Retroperitoneal Ganglioneuroma. MMJ. 2025, June. Vol 2 (2).
References
- Decarolis B, Simon T, Krug B, et al. Treatment and outcome of Ganglioneuroma and Ganglioneuroblastoma intermixed. BMC Cancer. 2016;27(16):542.
- Mylonas KS, Schizas D, Economopoulos KP. Adrenal ganglioneuroma: What you need to know. World J Clin Cases. 2017;5(10):373-77.
- Geoerger B, Hero B, Harms D, et al. Metabolic activity and clinical features of primary ganglioneuromas. Cancer. 2001;91(10):1905-13.
- Lonergan GJ, Schwab CM, Suarez ES, et al. Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma: radiologic-pathologic correlation. Radiographics. 2002;22(4):911-34.
- Rosai J. Rosai and Ackerman's Surgical Pathology. 11th Edition. Philadelphia: Elsevier; 2018. p. 1200-5.
- Mills SE, Carter D, Greenson JK, et al. Sternberg's Diagnostic Surgical Pathology. 8th Edition. Philadelphia: Wolters Kluwer; 2023. p. 654-61.
- Dumont RA, Hechelhammer L, Buck A, et al. Imaging of ganglioneuroma: diagnostic value of MRI and CT. AJR Am J Roentgenol. 2008;190(6):1410–15.
- Hayes FA, Green AA, Rao BN. Clinical manifestations of ganglioneuroma. Cancer. 1989;63(6):1211-14.