

Abstract:
Primary tumours of the female urethra are rare and account for less than 0.02% of malignant diseases in women. Management varies depending on the clinical stage and location of the lesion. Currently, there are no randomised studies to guide treatment of this disease. The purpose of this study is to report a case of squamous cell carcinoma (SCC) of the distal urethra (cT3N0M0) in a female, treated using an in-house developed, reusable, six channel vaginal brachytherapy cylinder. A 11 x 12 x 8 mm tumour, involving the anterior vagina and posterior urethral wall at the level of the external urethral meatus, was treated with 45 Gray (Gy) in 25 fractions to the gross disease and regional lymph nodes using external beam radiotherapy (EBRT), followed by intra-vaginal brachytherapy (IVBT) as a minimally invasive procedure. An IVBT planning scan was performed with a Foley catheter in situ, and contrast was instilled into the bladder, to displace the anterior urethral wall and bladder away from the target. An in-house developed six-channel applicator was used to deliver a targeted brachytherapy dose of 3 Gy per fraction (to a depth of 1.3 cm) for six fractions. The patient tolerated the procedure well, without significant side effects. Response assessment, conducted two months post-treatment using contrast-enhanced magnetic resonance imaging (CE-MRI), showed complete resolution of disease. The peripheral needle placement allowed for asymmetric dose shaping to adequately cover the target while minimising exposure to organs at risk. The use of commercially available multi-channel applicators’ is often limited by cost. However, our low-cost, in-house developed, multi-channel vaginal cylinder is reusable and can be applied across various clinical cases.
Key words: Brachytherapy, Multichannel Brachytherapy, Intra-Vaginal Cylinder, Carcinoma Urethra.
Introduction
Primary urethral carcinomas are exceedingly rare, more prevalent among men than in women, and account for less than 1% of all genitourinary malignancies.1 Among neoplasms of the female urethra, the majority (38%–46.7%) are adenocarcinomas. Less common histological types include squamous cell carcinoma (SCC; 25.4%–28%), urothelial carcinoma (24.9%–28%) and other variants (6%).2
Clinical management varies depending on the clinical stage and location of the lesion. To date, no prospective randomised studies exist to guide treatment. Both surgery and radiotherapy (RT) have been advocated as effective treatment modalities for early-stage urethral cancers.
Tumours arising from the distal urethra are generally diagnosed at an early stage and have high cure rates. However, knowledge about this rare disease remains limited, and most available data derive from individual case reports. We therefore present our case of female urethral carcinoma treated with RT
Case Report
A 72-year-old woman presented with dysuria and a burning sensation in the urethra. Clinical examination revealed a nodular lesion at the posterior aspect of the urethral meatus. The mass was palpable both at the urethral meatus and in the distal urethra on vaginal examination. Suspicious anterior vaginal wall involvement was noted, but no palpable inguinal lymphadenopathy was present (Figure 1). A contrast-enhanced magnetic resonance imaging (CE-MRI) scan of the pelvis showed a small, well-defined, T2 hyperintense cystic lesion (measuring 11 x 12 x 8 mm) in the left anterolateral aspect of the vagina, located below the level of pubic symphysis and at the level of the external urethral meatus. The lesion showed internal diffusion restriction and thin peripheral post-contrast enhancement (Figure 2). A biopsy was performed, and histopathology was suggestive of SCC. A whole body 18-fluorodeoxy-glucose (FDG) positron emission tomography-computed tomography (PET-CT) scan was done to rule out metastatic disease. It showed FDG-avid, mildly ill-defined thickening (maximum standardised uptake value [SUVmax] 8.1) in the distal vaginal canal, with no other abnormal hypermetabolic foci elsewhere in the body. The tumour was clinically staged as cT3N0M0, according to the American Joint Committee on Cancer (AJCC) 8th edition.3

Figure 1: Pre-treatment clinical image of the urethral meatus (lesion visible in posterior wall).

Figure 2: Pre-treatment axial section of T2-weighted magnetic resonance image of lesion (marked with arrow) in posterior urethra.
The case was discussed by a tumour board, and in view of the patient’s age and tumour stage, the consensus recommendation was to proceed with definitive RT. The patient received external beam radiotherapy (EBRT) to the gross tumour and regional lymph nodes with a total dose of 45 Gy delivered in 25 fractions (1.8 Gy per fraction) using image-guided intensity modulated radiation therapy (IGRT).
This was followed by intra-vaginal brachytherapy (IVBT). For optimal organ sparing, a planning scan was performed with a Foley catheter in situ and contrast introduced into the bladder to visualise and displace the anterior urethral wall and bladder away from the treatment field (Figure 3). A custom-designed, in-house developed six-channel applicator was used to deliver a targeted brachytherapy dose of 3 Gray (Gy) per fraction to a depth of 1.3 cm, delivered twice daily, at least 6 hours apart for a total of six fractions over three days. This applicator enabled differential dosing to the target volume while minimising exposure to the rectum and posterior vaginal wall (Figure 3). The patient tolerated the procedure well, without any significant side effects. The dose received by 2 cc volumes of the bladder and rectum was 0.7 Gy and 1.5 Gy per fraction, respectively. A total of 95% of the clinical target volume received 97% of the prescribed dose.
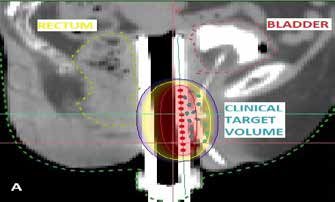


Figure 3: (A) Planned treatment isodose lines (75% – dark blue, 100% – yellow, 200% – red) covering the clinical target volume (dotted blue line) and sparing of the rectum (dotted yellow) and bladder (dotted red); (B and C) In-house developed six-channel intravaginal brachytherapy cylinder – (B) Individual components; (C) Assembled cylinder
Two months post-treatment, CE-MRI (Figure 4) showed a significant response to therapy, with no diffusion restriction noted in the urethral region, indicating a complete response. On clinical examination, no lesion was visible or palpable at the urethral meatus (Figure 5).

Figure 4: Post-treatment axial section of T2-weighted magnetic resonance image showing complete resolution of lesion (arrow marking pre-treatment disease location).

Figure 5: Post-treatment clinical image of the posterior urethral meatus (no visible lesion).
Discussion
The primary urethral carcinoma in females is a rare disease, with adenocarcinoma being the most common histological type, followed by SCC.2 Symptoms of female urethral carcinoma are varied, and the carcinoma initially spreads by local invasion into the periurethral tissue, vagina, vulva, and proximally to the bladder neck.3 Lymphatic drainage from the proximal urethra is to the obturator and internal iliac group of lymph nodes, while drainage from the distal urethra is to the inguinal group of lymph nodes. Up to 30% of patients have clinically palpable lymph nodes, and over 90% of these are metastatic. Distant metastasis is uncommon.3 Biopsy may be performed cystoscopically or transvaginally with a needle.
MRI is commonly used for staging, and treatment is determined by the stage at initial presentation. Bracken et al. observed 81 cases of female urethral carcinoma and found that patients with large tumours (>4 cm) had a lower 5-year survival rate (13%) compared to patients with small tumours (<2 cm, 60%).4 Given the poor prognosis associated with this cancer, knowledge of prognostic factors is essential.
Due to its rarity, establishing a definitive treatment strategy is challenging. A multimodal therapy approach which includes definitive surgery plus chemotherapy and RT is generally recommended. However, RT is an alternative to surgery in locally advanced disease, with comparable survival rates5 as shown in a large retrospective, registry-based study. The authors support the use of definitive RT (with or without chemotherapy) as a treatment option for organ preservation in well-selected patients.6 The addition of brachytherapy (BT) to RT reduces the risk of local recurrence,7 and in our case, the use of a six-channel IVBT cylinder allowed for differential dose distribution. This facilitated a dose escalation to the target area while minimising radiation to the adjacent organs, as compared to a standard single-channel applicator.
Conclusion
Although female urethral carcinoma is a rare disease entity, clinicians should maintain a high index of suspicion for malignancy in patients with relevant symptoms to make an accurate diagnosis. Careful clinical examination and imaging studies are helpful for confirming the diagnosis. Although there is no established standard therapy, RT combined with BT may be considered as an effective organ-preserving treatment option.
Rashi Agrawal, Nelesh Aggarwal, Balasubramanian S, Deepak Arora. A Rare Case of Female Urethral Carcinoma Treated with an In-house Developed Intra-Vaginal Brachytherapy Cylinder. MMJ. 2025, June. Vol 2 (2).
References
- Bracken RB, Johnson DE, Miller LS, et al. Primary carcinoma of the female urethra. J Urol. 1976;116(2):188–192.
- Aleksic I, Rais-Bahrami S, Daugherty M, et al. Primary urethral carcinoma: A Surveillance, Epidemiology, and End Results data analysis identifying predictors of cancer-specific survival. Urol Ann. 2018;10(2):170–174.
- Bhirud DP, Mittal A, Mavuduru RS, et al. Female distal urethral primary urothelial carcinoma: rare entity and management. Indian J Surg. 2021;83:582–4.
- Gatta G, van der Zwan JM, Casali PG, et al. Rare cancers are not so rare: the rare cancer burden in Europe. Eur J Cancer. 2011;47(17):2493–2511.
- Son CH, Liauw SL, Hasan Y, et al. Optimizing the Role of Surgery and Radiation Therapy in Urethral Cancer Based on Histology and Disease Extent. Int J Radiat Oncol Biol Phys. 2018;102(2):304–313.
- Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, Sullivan DC, Jessup JM. AJCC cancer staging manual. Amin MB, Edge SB, Greene FL, editors. New York: Springer; 2017 Jan.
- Milosevic MF, Warde PR, Banerjee D, et al. Urethral carcinoma in women: results of treatment with primary radiotherapy. Radiother Oncol. 2000;56(1):29–35.