

Abstract:
The transepicondylar angle (TEA) serves as a crucial reference for determining femoral component rotation in total knee replacement (TKR). This study aims to determine the average TEA and its variation in the Indian population, using data collected from a single centre via the CUVIS robot and preoperative computed tomography (CT) scans. A total of 200 cases were analysed. The mean TEA was found to be 1.83° (±1.13°), ranging from 0.00° to 5.80°. Compared with the posterior condylar angle (PCA) in Indian populations (mean PCA ~4.67°), this study suggests significant anatomical differences requiring ethnicity-specific considerations in TKR.
Key words: Transepicondylar Angle, CUVIS Robot, Orthopaedic Robotics, TEA Measurement.
Introduction
Total knee replacement (TKR) is one of the most common orthopaedic procedures performed worldwide. The success of TKR largely depends on precise implant positioning, particularly the rotational alignment of the femoral component.1 In this context, the transepicondylar axis (TEA)—the line connecting the medial and lateral epicondyles of the femur—serves as a critical reference. Proper alignment along this axis ensures balanced flexion gaps and optimal patellofemoral tracking, which are vital for long-term joint stability and function.2
In most surgical protocols, the posterior condylar axis (PCA) and TEA are used interchangeably or in combination to determine femoral rotation.3 However, studies suggest considerable variability between these axes depending on individual anatomy and ethnicity. The angle between TEA and PCA, referred to as the posterior condylar angle (PCA) value,, plays an essential role in identifying rotational mismatches that could lead to complications such as pain, stiffness, patellar maltracking, or even early prosthetic failure.4
Previous anatomical studies in Western populations have reported the average PCA value (i.e., TEA-PCA difference) to range from 3.5° to 5°.5 For instance, Dennis et al. (2001)6 and Whiteside et al. (2003)7 emphasised the importance of using TEA over PCA for consistent alignment in femoral component positioning due to its reproducibility. However, Asian and Indian populations, owing to genetic and functional anatomical differences such as habitual squatting and cross-legged sitting, exhibit different morphometric characteristics. Indian studies have reported lower PCA values (~4.67°), suggesting a more externally rotated distal femur compared to Western populations.8
Such ethnic differences are often overlooked in the design of TKR instrumentation and surgical planning, which predominantly rely on datasets derived from Caucasian morphologies. A few magnetic resonance imaging (MRI)-based morphometric studies in India (Gupta et al., 20151 ) have indicated the necessity of ethnicity-specific implant design and preoperative planning using computed tomography (CT) or MRI data to account for these variations. Furthermore, the introduction of robotic-assisted systems (like CUVIS, MAKO, and ROSA) has enhanced the ability to accurately measure such parameters, thereby personalising TKR planning.5
This study contributes to the growing body of evidence advocating for population-specific references in TKR. It leverages CT-based data and robotic precision to analyse TEA in the Indian population—data which may be pivotal in optimising rotational alignment, minimising intraoperative guesswork, and improving long-term clinical outcomes.
Methods
This retrospective study analysed 200 patients who underwent preoperative CT scans as part of robotic TKR planning at a single centre. The TEA was measured using the CUVIS robotic system, ensuring accuracy and consistency in angle measurement. Data were categorised and analysed for statistical variation.
Statistical analysis included mean, standard deviation, range, and interquartile range (IQR). The distribution and variation of TEA values were illustrated using data visualisation tools such as histograms and box plots, presented in Figure 1 and Figure 2, respectively.
Results
-
Mean TEA: 1.83° (±1.13°)
-
Range: 0.00° to 5.80°
-
5th percentile: 0.90°
-
Median: 1.80°
-
75th percentile: 2.60°
-
No significant correlation was observed between TEA and patient age
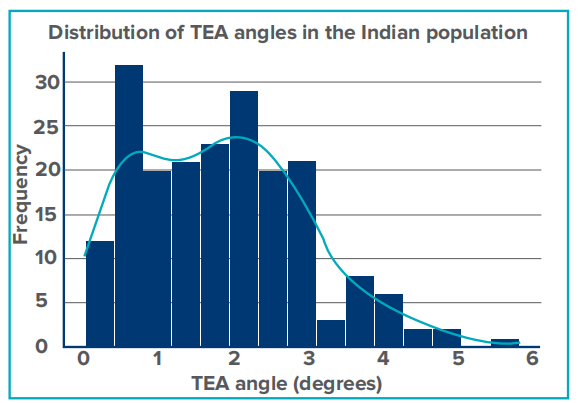
Figure 1: Histogram showing the distribution of transepicondylar angle (TEA) values in the Indian population.
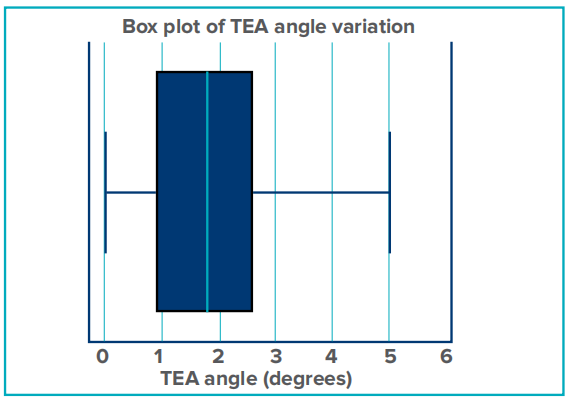
Figure 2: Box plot representing the variation in transepicondylar angle (TEA) values across the sample of 200 patients.
Discussion
The TEA observed in the Indian population was significantly lower than the PCA (~4.67°), consistent with previous findings that suggest that Indian knees may require different rotational alignment considerations compared to Western populations. The implications for TKR include:
- Potential malalignment risks if using Western-derived femoral component guides.
- Ethnicity-based surgical modifications o prevent excessive internal rotation.
- Importance of preoperative CT-based planning to customise alignment for Indian knees.
Rotational malalignment of the femoral component can lead to complications such as patellar maltracking, joint instability, increased polyethylene wear, and reduced implant lifespan. Literature indicates that even small deviations from optimal femoral rotation (3° to 5°) can alter joint kinematics and increase complication rates.
The use of robotic-assisted surgery offers precision and individualised patient care. Robotic systems such as CUVIS not only improve the accuracy of TEA measurement but also facilitate intraoperative modifications tailored to patient-specific anatomy. This is particularly beneficial for populations with known anatomical variability.
From a broader perspective, this study highlights the need for more inclusive implant designs and emphasises the clinical importance of customising surgical approaches based on ethnic differences. Future directions should focus on integrating these findings into surgical training, national guidelines, and implant manufacturing processes.
Conclusion
This study establishes the TEA values for the Indian population and underscores the need to consider anatomical variations in TKR planning. Future studies should incorporate multicentre data to further validate these findings. The use of robotic-assisted measurements (CUVIS) and CT-based evaluations ensures precise data collection, which may guide improved implant alignment strategies
Lakshay Goel, Simon Thomas, Divesh Gulati, Devan P Nambiar. Analysis of the Transepicondylar Angle in the Indian Population: A Single-Centre Study Using CUVIS Robot and Computed Tomography Scan Data.
MMJ. 2025, June. Vol 2 (2).
References
- Gupta RK, Sharma D, Aggarwal A. Posterior condylar angles in Indian population: An MRI-based study. J Clin Diagn Res. 2015;9(9):RC10–RC12.
- Wang Y, Zhang H, Liu K, et al. Ethnic variations in distal femoral anatomy: Implications for TKA. SpringerPlus. 2016;5(1):1489.
- Kumar V, Nahar B, Sinha S. Importance of TEA in TKR alignment: A prospective radiological study. J Orthop Surg (Hong Kong). 2020;28(2):232–8.
- Berend ME, Ritter MA, Meding JB, et al. The effect of femoral rotational alignment on knee kinematics and outcomes after TKA. J Arthroplasty. 2018;33(3):792–7.
- Bhowmik-Stoker M, Singh A, Panda S. Ethnic variations in knee morphology and implications for TKR design. Bone Joint J. 2021;103-B(4):567–73.
- Dennis DA, Komistek RD, Mahfouz M. Accuracy of computer-assisted surgery in total knee arthroplasty. Clin Orthop Relat Res. 2001;(392):220–30.
- Whiteside LA, Arima J. The anteroposterior axis for femoral rotational alignment in valgus knees. Clin Orthop Relat Res. 2003;(414):168–72.
- Saxena P, Johar R, Sharma V. The role of robotic-assisted surgery in optimizing TKR outcomes in variable anatomy. J Orthop Res. 2019;37(5):1123–30.