

Abstract:
Symptomatic aortic thrombosis is a devastating condition in the neonatal intensive care unit (NICU), which is now being increasingly diagnosed with the availability of bedside ultrasound. Early intervention can go a long way in preventing adverse outcomes. In our case, a preterm, very low birth weight, growth-restricted baby developed aortic thrombosis with hypertensive emergency and later limb-threatening ischaemia — which usually requires thrombolysis. However, due to parents’ reservations, he was given only therapeutic anticoagulation, with closely monitored activated partial thromboplastin time (APTT) targets, and this resulted in complete thrombus resolution. A multidisciplinary team approach was followed, and early detection with frequent monitoring led to a favourable outcome.
Key words: Neonatal Aortic Thrombosis, Thrombolysis, Heparin, Growth Restriction
Introduction
Neonatal thrombosis is an emerging, rare complication of tertiary care neonatology with more remarkable survival of preterm babies. Timely diagnosis requires a high index of suspicion so that life-threatening complications can be pre-empted. Also, given the very limited experience with anticoagulants and fibrinolytics in this age group, and the high risk of bleeding, therapy must be carefully tailored in each case. Here, we report a case of spontaneous arterial thrombosis in a sick preterm that presented as a hypertensive emergency with multi-organ dysfunction, diagnosed by Doppler ultrasound and successfully managed with unfractionated heparin (UFH) infusion.
Case Report
A male baby conceived by in vitro fertilisation, weighing 1412 g, was delivered at 32 weeks’ gestation via Caesarean section due to severe pregnancy-induced hypertension in the mother. The baby was the second of the dichorionic diamniotic twins and had features of foetal growth restriction. The mother had pregnancy-induced hypertension and intrahepatic cholestasis of pregnancy. There were no antenatal risk factors for sepsis. The baby cried immediately after birth but developed respiratory distress soon after, which was managed as per standard protocol after being shifted to the neonatal intensive care unit (NICU). The baby was started on orogastric feeds, which he did not tolerate, and had to be given fluids on Day 1 through a peripherally inserted central catheter (PICC) line. Initial investigations revealed thrombocytopenia (120000 per μL), polycythaemia (Haematocrit 66.4%), and a negative sepsis screen. Repeat haematocrit at 12 hours of life had reduced to 60%.
On Day 2 of life, the baby had recurrent desaturations and was started on caffeine citrate. Dobutamine infusion was initiated in view of transitional circulation. A repeat sepsis screen was positive, prompting the initiation of broad-spectrum antibiotics (piperacillin-tazobactam and amikacin). By Day 3, the baby was off respiratory and inotropic support. Minimal enteral feeds were restarted and gradually increased.
After the initial improvement in respiratory parameters, the baby abruptly developed an increased fraction of inspired oxygen (FiO2) requirement with poor perfusion and hypertension on Day 5. A repeat screen showed rising trend of C-reactive protein (CRP), leukopenia and worsening thrombocytopenia (platelet counts 61,000 per µL). Blood cultures from twin 1 (sent on Day 1) grew Klebsiella (sensitive to meropenem and amikacin); accordingly, antibiotics in this infant were escalated. However, blood culture of this baby (twin 2) remained sterile.
Functional echocardiography demonstrated severe left ventricular dysfunction with mild eccentric mitral regurgitation; a single dose of intravenous furosemide was given, and the baby was started on labetalol infusion.
On Day 6 of life, renal function started deteriorating but urine output was maintained and ultrasound of the kidney, ureter, and bladder (KUB) was normal. Doppler ultrasound revealed partial thrombosis of abdominal aorta (Figure 1) extending into left renal artery. Anticoagulation was started with subcutaneous low molecular weight heparin (LMWH) at a dose of 1.5 mg/kg/dose every 12 hours.

Figure 1: Doppler ultrasound showing partial thrombosis of the abdominal aorta.
On Day 7 of life, clinical signs of right lower limb ischaemia were noted (Figure 2a) in the form of pallor and absent pulses. Review Doppler revealed dampened flow in the right external iliac (Figure 2b) and common femoral arteries, with echogenic thrombus in the renal and infrarenal abdominal aorta and narrowing of the left renal artery ostium. Paediatric cardiology and cardiovascular surgery teams were consulted. In view of thrombus progression despite subcutaneous LMWH and potential limb-threatening complications, thrombolysis was discussed with parents; the higher risk of bleeding complications after thrombolysis, compared to adults, was also explained. Following detailed and informed discussion, they gave a negative consent at this stage. They reserved their right to revisit this issue after brief trial of alternate therapy.

Figure 2a: Ischaemic colour changes in the right lower limb on Day 7.

Figure 2b: Doppler showing dampened flow pattern in right external iliac artery.
As renal function was deranged and Factor Xa level monitoring was unavailable, LMWH was stopped, and UFH infusion was started via central line. Activated partial thromboplastin time (APTT) was monitored every six hours, targeting 2-2.5 times the control value. Limb inspection the next day showed some improvement in temperature and colour of the affected limb, but pulses were still palpable. Doppler showed no further thrombus extension; APTT-guided heparin infusion was continued.
Finally, by Day 10 of life, right lower limb perfusion was restored and Doppler showed normal flow in right external iliac artery (Figure 3a). Skin colour changes resolved by Day 12 (Figure 3b). On Day 13 of life, labetalol infusion was stopped, and he was shifted to oral amlodipine. Feed intolerance continued until Day 14, after which he started tolerating feeds. Antibiotics were stopped on Day 14 of life. Cranial ultrasound done twice between Days 6 and 8 did not show any evidence of intraventricular haemorrhage.
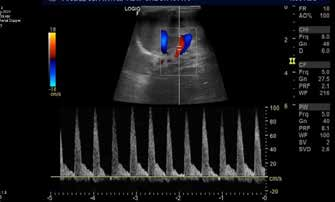
Figure 3a: Renal Doppler showing normalisation of flow.

Figure 3b: Perfusion restored in the right lower limb on Day 12 of life.
Ultrasound on Day 16 revealed thin filaments of thrombus suggestive of resolving thrombi. Renal function had normalised; UFH was stopped and switched to LMWH, which was continued until the thrombophilia workup was complete.
Blood pressure normalised, and amlodipine was stopped on Day 20 of life. Review Doppler on Day 22 revealed marked resolution of thrombus in the abdominal aorta, left renal artery, and right external iliac artery, with only thin residual filamentous thrombi.
Intravenous fluids were gradually tapered, and the baby was on full feeds by Day 24 of life when the PICC line was removed. On Day 27 of life, there was no more thrombus (Figure 4), and flow in affected vessels was normal; enoxaparin was stopped.

Figure 4: Thrombus completely resolved on Day 27.
Investigations
In addition to the relevant investigations and serial radiological tests, a detailed thrombophilia workup was done, which revealed normal functional activity of protein C and S and antithrombin III. Genetic studies for the methylene tetrahydrofolate reductase gene, prothrombin gene 20210A, and Factor V Leiden mutation were negative.
Differential Diagnosis
Causes for hypertensive emergency in a newborn may include renovascular (e.g., renal artery stenosis, renal vein thrombosis, acute kidney injury), cardiovascular, endocrine (e.g., congenital adrenal hyperplasia, hyperaldosteronism, hyperthyroidism), raised intracranial tension, or drugs (e.g., steroids, caffeine). Most of the aforementioned conditions were ruled out in our patient — although renal impairment did occur, it followed the hypertension rather than preceding it.
The baby had a few risk factors for neonatal thrombosis, including prematurity, intrauterine growth restriction, and a positive sepsis screen. However, these are more commonly associated with arterial thrombosis in the presence of underlying thrombophilic conditions — for which the baby tested negative. Moreover, in the absence of an umbilical artery catheter, arterial thrombosis manifesting as symptomatic aortic thrombosis was unexpected.
Treatment
A multidisciplinary team monitored the patient, and the baby’s parents were involved in the decision-making process regarding anticoagulation versus thrombolysis at a crucial stage.
Outcome and Follow-Up
The baby was discharged on Day 28 of life on full breastfeeds, with adequate weight gain, a normal neurological examination, and a normal pre-discharge cranial ultrasound. Extensive thrombophilia workup was negative, and no antiplatelet or anticoagulant was prescribed at discharge. The baby remains under regular follow-up and is thriving. At 1 year of age, the child has no hypertension, no limb length discrepancy, and no functional deficit.
Discussion
Thrombosis is more common in the neonatal period than at any other age during childhood.1 Improved survival of sick and preterm infants has led to increased diagnosis in recent years. Arterial thromboses constitute nearly 50% of all neonatal thrombotic events, with an overall incidence of 5.1 per 100000 live births and 0.2% of NICU admissions. The largest study reported an incidence of 2.4 per 1000 admissions.2-4 However, symptomatic aortic thrombosis remains exceedingly rare (0.1 to 1.1 per 100000 live births).4
Neonates have increased inherent vulnerability for both haemorrhage and thrombosis due to altered thrombogenic and fibrinolytic pathways. This liability is due to reduced synthesis of various coagulation proteins, increased clearance of the coagulation factors, and altered function of certain factors and platelets.5
In some reports, the umbilical arterial catheter is the most critical risk factor for arterial thrombosis, with an incidence as high as 63%.6 Other known risk factors include sepsis, prematurity, asphyxia, dehydration, polycythaemia, and maternal diabetes. Less commonly, deficiencies of antithrombin III, protein C, protein S, as well as genetic defects like activated protein C resistance, Factor V Leiden mutation, hyperhomocysteinaemia, elevated lipoprotein (a), and the prothrombin gene G20210A mutations have been implicated. These genetic predispositions may have additive effects if other risk factors are present in a baby. In this case, the baby was growth-restricted, a factor that has also been proposed as a potential contributor to thrombosis, particularly in those with underlying prothrombotic conditions.7 Another important aspect is the maternal presence of autoantibodies, such as antiphospholipid antibodies, which can also predispose neonates to thrombosis, suggesting a need to screen such babies for these antibodies during the neonatal period.8
Aortic thrombosis can present variably, ranging from asymptomatic to severe life-threatening complications, depending on the site and degree of occlusion by thrombus. This has been detected incidentally on autopsy of neonates who died due to some other reasons — especially in association with catheters. Initial presentation can include decreased distal pulsations and inability to withdraw blood from the catheter.9 Other signs can be colour change, peripheral gangrene, blood pressure difference between upper and lower limbs, renal failure, necrotising enterocolitis, congestive cardiac failure, and hypertension, to name a few.
The diagnostic approach to thrombosis varies. Angiography, although the gold standard for diagnosis of thrombosis in adults, is rarely used in neonates due to procedural difficulty. Ultrasound Doppler is the preferred modality whenever there is clinical suspicion of thrombosis; however, this may underdiagnose this condition. Echocardiography is indicated if cardiac dysfunction is suspected.
Symptomatic aortic thrombosis necessitates immediate triaging based on severity to determine the appropriate level of treatment to be initiated. It also depends on the centre’s capabilities. The aim of the therapy in any case is to reduce further extension of the thrombus, restoration of blood flow to the affected organs, and reduce the risk of recurrence.10
LMWH is the preferred anticoagulant in neonates because it has less risk of thrombocytopenia, a more predictable pharmacokinetic profile, requires minimal monitoring and subcutaneous administration.11 UFH is an alternative for anticoagulation, but it causes thrombocytopenia, requires frequent monitoring, has a short half-life, and may have partial resistance due to low antithrombin levels. In that case, plasma transfusion is required to replete levels of antithrombin. These anticoagulants have equal efficacy in studies, and the decision is usually individualised.
Thrombolytic therapy includes agents like streptokinase, urokinase, and recombinant tissue plasminogen activator (tPA). However, the low plasminogen concentration in neonates may decrease the efficacy of these agents.11 Conversely, immature cerebral vessels predispose to an increased risk of bleeding. Although systemic thrombolysis is a well-described treatment option for symptomatic thrombosis, there is very limited data in neonates. In an old review, thrombolytic patency rates in neonates were reported to be 39% to 86%.12 This was a combined study using all three agents. Recombinant tPA (Alteplase) is the preferred drug in neonates for thrombolysis as it has better clot lysis, increased fibrin specificity, fewer allergic reactions and shorter half-life. Prior administration of plasminogen through fresh frozen plasma (FFP) is recommended to augment its action.13 Thrombolysis is associated with haemorrhagic complications and distal limb ischaemia due to distal embolisation.
Surgical thrombectomy is an option in managing neonatal aortic thrombosis, but is rarely used owing to the surgical risks and limited data availability in the neonatal population. A case series by Payne et al.14 described aortic thrombosis in 12 neonates. Five of these patients were surgically treated with 100% survival. A Cochrane review comparing thrombolysis and surgical thrombectomy does not favour either approach in terms of limb salvage, amputation, or death and recommends that the choice between the two be individualised, balancing the risks of surgery against the potential complications of thrombolysis.15
An algorithmic approach has been suggested by Colburn et al.16 wherein all neonates with symptomatic aortic thrombosis should be given therapeutic anticoagulation. Further, if the neonate has absent distal pulses, then thrombolysis is initiated when there is no improvement in clot burden. Conversely, if the baby has gangrene or tissue loss features, thrombolysis is started immediately, and surgery is done if thrombolysis is unsuccessful. Upfront surgery is only suggested in neonates where thrombolysis is contraindicated. Constant Doppler monitoring is indicated to detect clot propagation for early escalation of care.
To conclude, symptomatic aortic thrombosis is a devastating complication rarely encountered in the NICU, even without an umbilical artery catheter. It needs a high index of suspicion for early detection and timely therapy. Anticoagulation remains the mainstay of treatment, with severe cases requiring thrombolysis or surgical thrombectomy. Timely intervention can drastically improve outcomes in affected neonates.
Conclusion
- Symptomatic aortic thrombosis is a rare complication in the NICU and requires a high index of suspicion, even in absence of umbilical catheter.
- Early detection and timely intervention can save babies from limb and life-threatening complications of aortic thrombosis.
- Therapeutic anticoagulation, when initiated early, appears to be safe and effective in neonates.
- Multidisciplinary evaluation and management, as well as shared decision-making involving the parents, contribute to better outcomes. Shared decision-making becomes especially important given the limited experience, high bleeding risk and possibly reduced efficacy of fibrinolytic therapy in newborns.
Kaushaki Shankar, Bhavya Kukreja, Vishnu D Aggarwal, Vandana Pandey, Saumya Shrivastava. Symptomatic Aortic Thrombosis in a Preterm Neonate: 1-Year Follow-Up. MMJ. 2025, June. Vol 2 (2).
References
- Motta M, Bagna R, Saracco P, et al. Neonatal thrombosis. Minerva Pediatr. 2010 Jun;62(3 Suppl 1):117–20.
- Schmidt B, Andrew M. Neonatal thrombosis: report of a prospective Canadian and international registry. Pediatrics. 1995;96(5 Pt 1):939–43.
- Robinson V, Achey MA, Nag UP, et al. Thrombosis in infants in the neonatal intensive care unit: Analysis of a large national database. J Thromb Haemost JTH. 2021;19(2):400–7.
- Nowak-Göttl U, von Kries R, Göbel U. Neonatal symptomatic thromboembolism in Germany: two year survey. Arch Dis Child Fetal Neonatal Ed. 1997;76(3):F163–167.
- Bacciedoni V, Attie M, Donato H, et al. Thrombosis in newborn infants. Arch Argent Pediatr. 2016;114(2):159–66.
- Rizzi M, Goldenberg N, Bonduel M, et al. Catheter-Related Arterial Thrombosis in Neonates and Children: A Systematic Review. Thromb Haemost. 2018;118(6):1058–66.
- von Kries R, Junker R, Oberle D, et al. Foetal growth restriction in children with prothrombotic risk factors. Thromb Haemost. 2001;86(4):1012–6.
- Bitsadze V, Nalli C, Khizroeva J, et al. APS pregnancy - The offspring. Lupus. 2020;29(11):1336–45.
- Bryant BG. Drug, fluid, and blood products administered through the umbilical artery catheter: complication experiences from one NICU. Neonatal Netw NN. 1990;9(1):27–32, 43–6.
- Makatsariya A, Bitsadze V, Khizroeva J, et al. Neonatal thrombosis. J Matern Fetal Neonatal Med. 2022;35(6):1169–77.
- Greenway A, Massicotte MP, Monagle P. Neonatal thrombosis and its treatment. Blood Rev. 2004;18(2):75–84.
- Nowak-Göttl U, Auberger K, Halimeh S, et al. Thrombolysis in newborns and infants. Thromb Haemost. 1999;82 Suppl 1:112–6.
- Monagle P, Chan AKC, Goldenberg NA, et al. Antithrombotic Therapy in Neonates and Children. Chest. 2012;141(2):e737S–e801S.
- Payne RM, Martin TC, Bower RJ, et al. Management and follow-up of arterial thrombosis in the neonatal period. J Pediatr. 1989;114(5):853–8.
- Darwood R, Berridge DC, Kessel DO, et al. Surgery versus thrombolysis for initial management of acute limb ischaemia. Cochrane Database Syst Rev. 2018;2018(8).
- Colburn MD, Gelabert HA, Quiñones-Baldrich W. Neonatal aortic thrombosis. Surgery. 1992;111(1):21–8.