

Abstract:
Pudendal neuralgia is a rare, chronic and debilitating pain syndrome affecting the sensitive areas of the body innervated by pudendal nerve. However, due to lack of awareness, most patients are frequently misdiagnosed or underdiagnosed by healthcare providers, including gynaecologists. Patients often go through multiple consultations with physicians of various disciplines, undergo multiple evaluations, and experience years of delay in diagnosis, resulting in significant delay in appropriate treatment. Consequently, those affected have a severely compromised quality of life and often develop mental health problems. They may suffer from depression or anxiety, accompanied by feelings of frustration, loneliness, and shame, and some may resort to suicide. Therefore, there is an urgent need for approaches towards growing awareness of the seriousness of this disease among gynaecologists.
Key words: Pudendal Neuralgia, Pudendal Nerve Entrapment Syndrome, Alcock Canal Syndrome, Neuropathy, Chronic Pelvic Pain, Nantes’ Criteria, Pudendal Nerve Block, Pudendal Decompression.
Introduction
Pudendal neuralgia is a chronic neuropathic pelvic and perineal pain syndrome that originates from injury, inflammation, or irritation of the pudendal nerve. It is also called the Alcock canal syndrome or pudendal nerve entrapment syndrome. As estimated by the International Pudendal Neuropathy Foundation, the incidence of this condition is 1 per 100,000, but the actual prevalence is believed to be substantially higher than reported.1 Pudendal nerve entrapment syndrome may affect 1% of the general population and accounts for about 4% of all patient consultations for pain control in chronic pelvic pain, with women affected more than twice as often as men.2 Primary symptoms of pudendal neuralgia include pelvic pain, sexual dysfunction and difficulty with urination or defaecation.3
Pelvic pain:
There is pain or an altered sensation in the dermatomal distribution of the pudendal nerve, including the vulva, clitoris, perineum and rectum. The pain typically occurs with sitting, especially on a hard surface, and improves on standing or in a lying-down position.4 The pain is typically unilateral and rarely occurs on both sides. Patients often describe the pain as a shooting, burning, pricking or tingling sensation.
Sexual dysfunction:
Women with pudendal neuralgia may experience decreased sensation in the genitals, perineum, or rectum. It may be difficult or impossible for the woman to achieve orgasm. At times, the patient may also present with painful nocturnal orgasms and persistent sexual arousal.5
Difficulty with urination/defaecation:
Patients may experience urinary hesitancy, urgency and/or frequency. They may feel that they have to ‘strain’ to have a bowel movement and might have pain or discomfort after a bowel movement. Constipation is also common among these patients. In severe cases, complete or partial urinary and/or faecal incontinence may result.5,6
The sensation of a foreign object:
Some patients feel as though there is a foreign object sitting inside the vagina or the rectum. Some describe it as “sitting on a marble” or “having something stuck inside.”7
Aetiology
The cause of pudendal neuralgia lies in its peculiar anatomy, which makes it susceptible to compression and entrapment, leading to nerve dysfunction and consequent symptoms. Other causes of pudendal neuralgia have also been described in the literature, like compression by a malignant or benign tumour, trauma at the sacral or nerve root level, stretching and lengthening of the nerve, followed by inflammation in situations like childbirth, repetitive straining during defaecation in case of constipation, squatting with heavy weights, etc.1,3
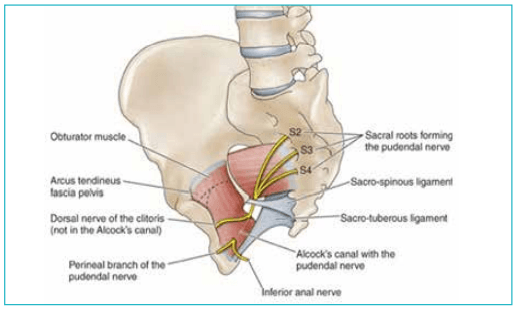
Figure 1: Course of the pudendal nerve. The nerve has a unique path in which it quickly exits the pelvis through the greater sciatic foramen inferior to the piriformis muscle. It then passes medially through the lesser sciatic foramen, enters the perineal region, and travels along the lateral wall of the ischioanal fossa in the pudendal canal (Alcock’s canal).
Anatomy of the Pudendal Nerve
The pudendal nerve is a mixed nerve carrying motor and sensory fibres from the ventral nerve roots of S2, S3, and S4. The nerve travels anterior to the piriformis muscle, squeezing between it and the coccygeus muscle through the greater sciatic foramen and between the sacrotuberous and sacrospinous ligaments. The net effect is analogous to a "clamp" or "lobster claw," pinching or impinging on the nerve.8 Upon leaving this site, the nerve travels through Alcock's canal (also known as the pudendal canal). It divides into the deep and superficial perineal nerves, the dorsal nerve of the penis or clitoris, and the inferior rectal nerve (Figures 1–3).6,8,9
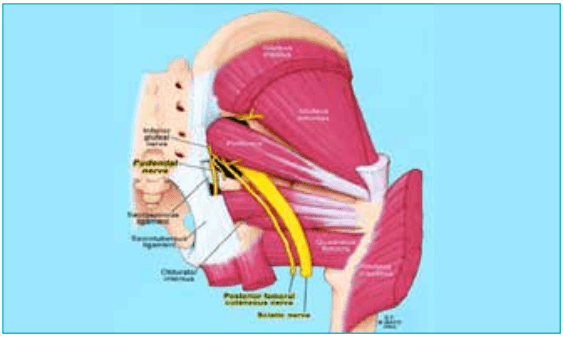
Figure 2: Pudendal nerve enters the gluteal region medial to the sciatic nerve, superficial to the sacrospinous ligament and deep to the sacrotuberous ligament. After coursing around the sacrospinous ligament, the pudendal nerve re-enters the pelvis through the lesser sciatic foramen.
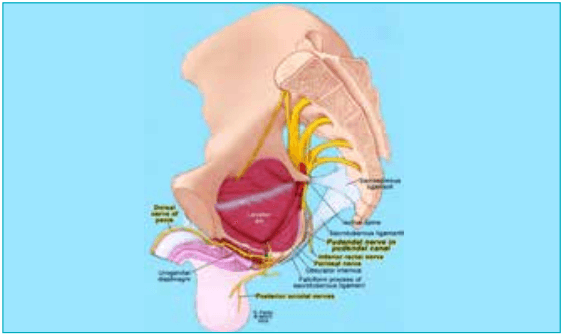
Figure 3: Pudendal nerve through the pudendal canal. Within the canal, the nerve splits into its 3 terminal branches, i.e. the inferior rectal nerve, the perineal nerve, and the dorsal nerve of the clitoris/penis. The inferior rectal nerve provides motor innervation to the external anal sphincter and surrounding levator ani muscles. It also provides sensory innervation to the skin of the anal triangle. The perineal nerve provides motor innervation to the transverse perinei muscle, the bulbospongiosus muscle, and the ischiocavernosus muscle, as well as to the external urethral sphincter. Finally, the dorsal nerve of the clitoris/penis travels parallel to the ischiocavernosus muscle and enters the clitoris/penis, providing innervation to the glans of each structure.
Pudendal neuralgia is caused by various mechanisms, which can be separated into three basic categories:4
1. As described, the pudendal nerve is anatomically vulnerable to compression and entrapment along its course (Figure 1). Patients with anatomical predispositions (i.e. smaller canals, a narrow window between ligaments, etc.) or biomechanical abnormalities are more susceptible to compression injuries. Patients may have a silent or asymptomatic compression for an extended period until an exacerbating and inflaming factor, such as surgery, haematoma, cycling, prolonged sitting, stress and tension-holding patterns, horseback riding, etc., causes entrapment, nerve dysfunction and symptoms.
Four common sites of pudendal nerve entrapment are described below:9
- Type I: Entrapment below the piriformis muscle as the pudendal nerve exits the greater sciatic notch
- Type II: Entrapment between sacrospinous and sacrotuberous ligaments (this is the most common cause of pudendal nerve entrapment)
- Type III: Entrapment within Alcock's canal
- Type IV: Entrapment of terminal branches only (inferior rectal nerves, superficial and deep perineal nerves, and the dorsal nerve of the penis/clitoris)
2. Sacral or radicular type: Factors such as benign or malignant tumours and trauma to the area may cause nerve compression or inflammation at the sacral or nerve root level.3,11
3. The pudendal nerve is also vulnerable to tension injuries. A variety of factors including vaginal childbirth, constipation with repetitive straining to defaecate, and squatting with heavy weights, can put undue tension on the nerve, causing it to lengthen beyond its normal limits and resulting in neural inflammation.13
Diagnosis
The diagnosis of pudendal neuralgia by pudendal nerve entrapment syndrome is essentially clinical. A clinical diagnostic criterion was discussed and published by a multidisciplinary working party in Nantes, France, in 2006.10 The "Nantes" inclusion criteria are shown in Table 1.
- Pain correlates with the anatomical distribution of the pudendal nerve
- Pain is predominantly in the sitting position
- The patient does not get up at night due to pain
- There is no identifiable sensory loss
- Relief of pain occurs with a pudendal nerve block
Diagnostic Criteria for Pudendal Neuralgia by Pudendal Nerve Entrapment
Nantes criteria,
Essential criteria (must all be present)
- Pain in the territory of the pudendal nerve: from the anus to the penis or clitoris
- Pain is predominantly experienced while sitting
- The pain does not wake the patient at night
- Pain with no objective sensory impairment
- Pain relieved by diagnostic pudendal nerve block
Exclusion criteria
- Exclusively coccygeal, gluteal, pubic or hypogastric pain
- Pruritus
- Exclusively paroxysmal pain
- Imaging abnormalities able to account for the pain
Complementary diagnostic criteria
- Burning, shooting, stabbing pain, numbness
- Allodynia or hyperpathia
- Rectal or vaginal foreign body sensation (sympathalgia)
- Worsening of pain during the day
- Predominantly unilateral pain
- Pain triggered by defaecation
- Presence of exquisite tenderness on palpation of the ischial spine
- Clinical neurophysiology findings in men or nulliparous women
Associated signs not excluding the diagnosis
- Buttock pain on sitting
- Referred sciatic pain
- Pain referred to the medial aspect of the thigh
- Suprapubic pain
- Urinary frequency and/or pain on a full bladder
- Pain occurring after ejaculation
- Dyspareunia and/or pain after sexual intercourse
- Erectile dysfunction
- Normal clinical neurophysiology
Table 1: Nantes criteria for diagnosis of pudendal neuralgia. analytes across the months using PreciControl Clinical Chemistry (PCCC1) in Cobas Pro with TIQCon Quality Performance software.5
Source: Labat J-J, et al. Neurourol Urodyn. 2008;27(4):306–10.10
When pudendal neuralgia due to pudendal nerve entrapment is diagnosed according to the Nantes criteria, no further investigation is required, and medical or surgical treatment can be proposed. Nevertheless, a number of other possible causes of pudendal neuralgia, like benign or malignant pelvic tumours, endometriosis, neuroma, pelvic floor dysfunction, genital prolapse, etc., must not be overlooked.11 However, a study conducted by Indraccolo et al. showed that atypical presentation of pudendal neuralgia (i.e. other than pudendal nerve entrapment) in females is low when clinical criteria for pudendal entrapment syndrome are applied. Hence, pudendal neuralgia has come to be used interchangeably with pudendal nerve entrapment and Alcock canal syndrome.
Management
Conservative:
Avoidance of painful stimuli is one of the most important components of treatment. For instance, if cycling causes pain, the patient should use proper padding or cease the activity. Other activities to avoid might be hip flexion exercises, jogging, rowing and gymnastics. Roughly 20%–30% of patients see relief from conservative measures alone.7
Physical therapy:
Pelvic floor physical therapy works best for patients in whom pain results from muscle spasms. Physical therapy releases spasms and relaxes pelvic floor muscles, thereby causing muscle lengthening. A course of 6–12 weeks is commonly recommended. Adding transcutaneous electrical nerve stimulation (TENS) to physical therapy appears to be helpful.12
Pharmacologic therapy:
There are no randomised trials to study and evaluate the efficacy of these drugs or which combinations might be most effective. Often, several medications from different drug classes are used. A typical combination would be a tricyclic antidepressant (amitriptyline), a serotonin–norepinephrine reuptake inhibitor (duloxetine), and a neurotransmitter analogue (gabapentin and/or pregabalin).7,13
Pudendal nerve block:
Infiltration with a local anaesthetic or steroid in an area encircling the pudendal nerve is the mainstay of pudendal nerve pain management. The block can be given unguided or with the aid of ultrasonography, fluoroscopy, or computed tomography (CT). While no standard medication or combination is used, one frequently used mixture includes 1% lidocaine, 0.25% bupivacaine, and a corticosteroid such as triamcinolone. About 25% of patients report pain relief lasting more than one month following pudendal nerve blocks.7 While this can be effective, there is evidence that ongoing therapeutic pudendal blocks may lose efficacy after two years.13
Surgical decompression:
Surgery to directly free the pudendal nerve in Alcock's canal is considered the most effective long-term treatment and potential cure for pudendal nerve entrapment. The four different approaches are transperineal, transgluteal, transischiorectal, and laparoscopic.14 Overall success with surgical decompression is about 70% (60%–80%).15 The goal of decompressive surgery is to completely free the nerve from entrapment and compression while allowing it complete mobility. Laparoscopy has the advantage of a better visual surgical field with built-in magnification. It allows for the option of leaving a neuromodulation electrode in place as a backup.15
Sacral neuromodulation:
This minimally invasive treatment includes using a peripheral nerve stimulator, which causes neural regulation of the pudendal nerve in the ischioanal fossa. It has often been used as a treatment of last resort when patients have failed all other treatments, including surgical decompression.2
Pulsed radiofrequency ablation, cryotherapy and lipofilling are relatively newer experimental methods of treatment of pudendal neuralgia.2
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
Conclusion:
Lack of awareness on the part of physicians, including the gynaecologists, about pudendal neuralgia has a severe negative impact on the quality of life of those suffering from it. Approaches like conducting workshops with the aim to impart extensive training on the anatomy of pelvic nerves and the ways to perform examinations specifically designed to evaluate the pudendal nerve may help in the diagnosis and management of this neuropathic pain. A multidisciplinary approach involving gynaecologists, urologists, colorectal surgeons, physical therapists and pain management specialists for the management of pudendal neuralgia should be encouraged to improve outcomes for the patients. Resources like the Health Organisation for Pelvic Education (HOPE) and the International Pelvic Pain Society (IPPS) aim to provide information and support to both patients and healthcare providers to bridge the knowledge gap.
Dhiranjali Sahoo, Bijoy Nayak. Pudendal Neuralgia: What Does a Gynaecologist Need to Know? MMJ.
2026, March. Vol 3 (1).
References
- Hibner M, Desai N, Robertson LJ, et al. Pudendal neuralgia. J Minim Invasive Gynecol. 2010;17(2):148–53.
- Guo KK, Wang L, Liu F, et al. Sacral nerve stimulation in patients with refractory pudendal neuralgia. Pain Physician. 2022;25(4):E619–E627.
- Filler AG. Diagnosis and treatment of pudendal nerve entrapment syndrome subtypes: imaging, injections, and minimal access surgery. Neurosurg Focus. 2009;26(2):E9.
- Ramsden CE, McDaniel MC, Harmon RL, et al. Pudendal nerve entrapment as source of intractable perineal pain. Am J Phys Med Rehabil. 2003;82(6):479–84.
- Waldinger MD, Venema PL, van Gils AP, et al. New insights into restless genital syndrome: static mechanical hyperesthesia and neuropathy of the nervus dorsalis clitoridis. J Sex Med. 2009;6(10):2778–87.
- Shafik A, El Sibai O, Shafik IA, et al. Role of sacral ligament clamp in the pudendal neuropathy (pudendal canal syndrome): results of clamp release. Int Surg. 2007;92(1):54– 59.
- Levesque A, Bautrant E, Quistrebert V, et al. Recommendations on the management of pudendal nerve entrapment syndrome: A formalised expert consensus. Eur J Pain. 2022;26(1):7–17.
- Bautrant E, de Bisschop E, Vaini-Elies V, et al. Modern algorithm for treating pudendal neuralgia: 212 cases and 104 decompressions. J Gynecol Obstet Biol Reprod (Paris). 2003;32(8 Pt 1):705–12.
- Kaur J, Leslie SW, Singh P. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 21, 2023. Pudendal Nerve Entrapment Syndrome.
- Labat JJ, Riant T, Robert R, et al. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol Urodyn. 2008;27(4):306–10.
- Ploteau S, Cardaillac C, Perrouin-Verbe MA, et al. Pudendal neuralgia due to pudendal nerve entrapment: Warning signs observed in two cases and review of the literature. Pain Physician. 2016;19(3):E449–54.
- Eid MM, Rawash MF, Sharaf MA, et al. Effectiveness of transcutaneous electrical nerve stimulation as an adjunct to selected physical therapy exercise program on male patients with pudendal neuralgia: A randomized controlled trial. Clin Rehabil. 2021;35(8):1142–50.
- Leslie SW, Antolak S, Feloney MP, et al. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Nov 28, 2022. Pudendal Neuralgia.
- Basol G, Kale A, Gurbuz H, et al. Transvaginal pudendal nerve blocks in patients with pudendal neuralgia: 2-year follow-up results. Arch Gynecol Obstet. 2022;306(4):1107–16.
- Erdogru T, Avci E, Akand M. Laparoscopic pudendal nerve decompression and transposition combined with omental flap protection of the nerve (Istanbul technique): technical description and feasibility analysis. Surg Endosc. 2014;28(3):925–32.