

Abstract:
Despite the availability of several classes of drugs, uncontrolled hypertension (HT) remains a challenge and is a significant contributor to cardiovascular (CV) morbidity and mortality. In most instances, this is due to inadequate dosing, side effects, non-compliance with medication, or failure to observe lifestyle changes. However, there are many patients for whom, despite all measures, the blood pressure (BP) continues to be high. Newer techniques such as renal denervation have been advocated, but different trials have given conflicting results. Several new classes of drugs have become available or are in different stages of clinical trials. Sacubitril/valsartan (s/v), a well-established drug for heart failure (HF) has been shown to be a powerful antihypertensive agent and is approved for this indication in some countries. Among the other emerging drugs, aldosterone synthase inhibitors (ASIs) appear promising, but more data are needed before they can be recommended for clinical use.
Key words: Hypertension (HT), Antihypertensive Drugs, Aldosterone Synthase Inhibitors.
Introduction
Hypertension (HT) is the commonest cardiovascular (CV) disease and contributes significantly to the morbidity and mortality. Estimates of its prevalence vary in different countries, but it is recognised that its incidence is higher in the middle- and low-income countries. The Fifth National Family Health Survey conducted in 2020-21 among 1,691,036 individuals, showed that 28.1% had hypertension, of whom only 36.9% were diagnosed.1 Of these, 44.7% were receiving treatment, and among them, only 52.5% had a blood pressure (BP) below 140/90 mmHg.
The use of double or triple drug combinations can help improve compliance in many of these patients. Recent guidelines recommend initiating treatment with a reninangiotensin-aldosterone system (RAAS) inhibitor along with a calcium channel blocker, with the addition of a thiazide diuretic if BP remains high. Further additions, including mineralocorticoid receptor antagonists (MRAs) and other drugs such as beta blockers, alpha blockers, loop diuretics, and clonidine may be required if HT remains uncontrolled. Renal denervation is another strategy that has had a chequered trajectory but can be considered in truly resistant HT (RHT).
Various preventive and treatment strategies are available; however, there remains a significant lack of awareness regarding the serious implications of uncontrolled HT in the population and the medical community. Even if the available strategies are diligently employed, there are always patients whose BP remains uncontrolled, and there is a need for developing newer therapies which can help these patients Therefore, as in all other branches of medicines, the quest for newer, more effective, and safer treatments continues.
Several novel drugs are now available or under investigation to address true RHT. This review focuses on the following emerging strategies which act through different pathways.
- New use for heart failure (HF) drug: Angiotensin receptorneprilysin inhibitor (ARNI)
- Aldosterone synthase inhibitors (ASI): Baxdrostat
- Messenger ribonucleic acid (mRNA) interference drug: Zilbesiran
- Inhibitor of aminopeptidase A (APA): Firibastat
- Endothelin antagonist: Aprocitentan
- Vaccines
Angiotensin Receptor-Neprilysin Inhibitor (ARNI)
ARNI is now a well-established drug for the treatment of HF, but was originally developed as a treatment for HT. This is not surprising, considering its powerful vasodilator action and other mechanisms by which it lowers BP. In fact, the first trial assessing its efficacy in the management of HT was published well before the landmark PARADIGM trial for heart failure with reduced ejection fraction (HFrEF). In 2010, 1215 patients were enrolled and over an 8-week treatment period, there was a greater reduction of BP with sacubitril/valsartan (s/v) vs valsartan (Figure 1). However, it was not pursued as an antihypertensive agent at that time.2
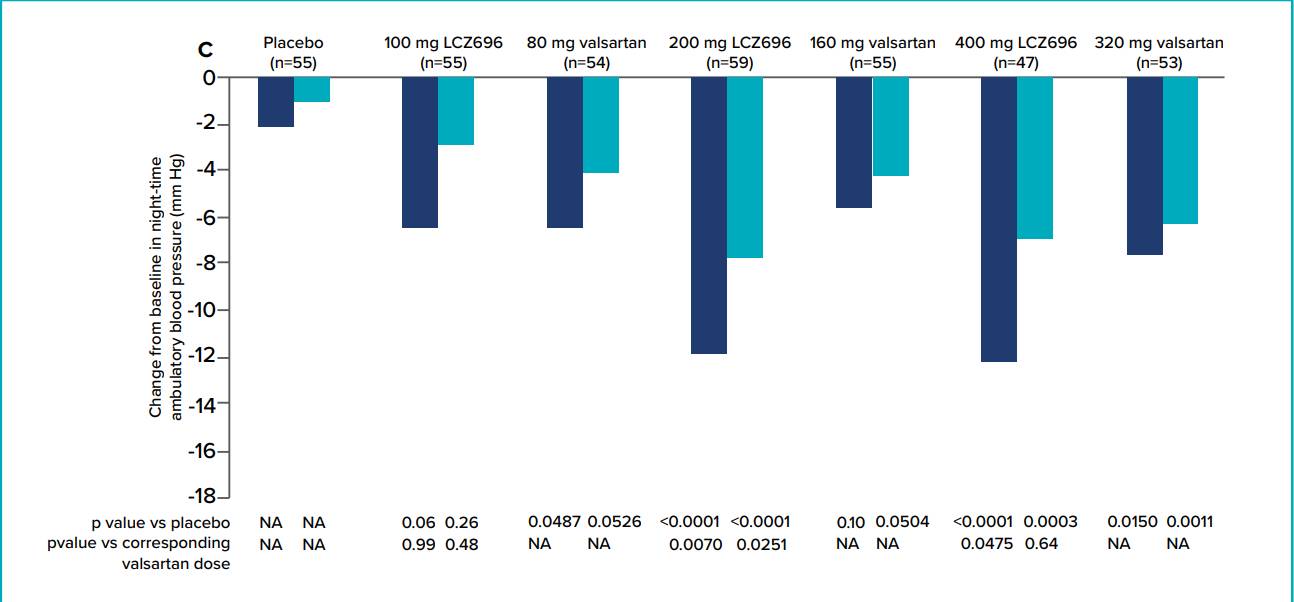
Figure 1: Blood-pressure reduction with LCZ-696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: a randomised, double-blind, placebo-controlled, active comparator study. Luis Miguel Ruilope, Andrej Dukat, Yves Lacourciere, Jianjian Gong, Martin P Lefkowitz. The Lancet. 2010;375(9722):1255-1266.
PARAMETER3 was the first randomised trial comparing s/v versus an angiotensin-receptor blocker (ARB), olmesartan on central aortic pressures and haemodynamics in elderly patients. It showed that s/v was significantly more effective than conventional ARB in lowering brachial and central aortic systolic pulse pressures (Figure 2).
In the post-hoc analysis of PARAGON-HF4 trial, the effect of s/v in patients with apparent RHT was compared with valsartan. In the 731 patients analysed, the reduction in BP was greater with s/v when compared to valsartan at both Week 4 and Week 16. The difference was more prominent in MRA-resistant HT. Sacubitril/valsartan has also been shown to reduce arterial stiffness more than ARBs which may be important in RHT.
A lack of a nocturnal dip in BP is an important risk factor in patients with HT. In a study of 632 in Japan patients conducted by Kazuomi Kario,5 ambulatory blood pressure monitoring (ABPM) was carried at baseline and at followup to compare the effect of s/v versus olmesartan. The study demonstrated that changes in 24 hours daytime and nighttime ambulatory systolic BP (SBP) and diastolic BP (DBP) were more significant with s/v compared to olmesartan. The effect was even pronounced in non-dippers as compared to dippers. Such an effect is likely to be useful in preventing future CV events. The drug is already approved in treatment of HT in Japan and China and is likely to be approved in other countries as well.
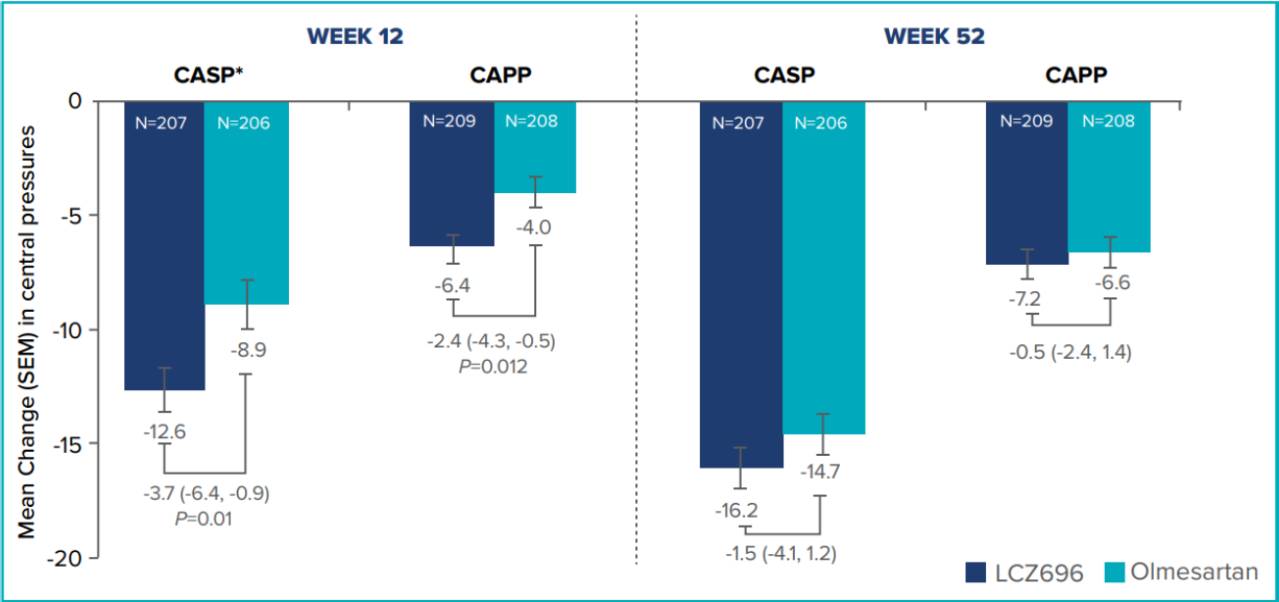
Figure 2: Effects of sacubitril valsartan versus olmesartan on central haemodynamics in the elderly with systolic hypertension. Bryan Williams, John R. Cockcroft, Kazuomi Kario, et al. Hypertension. 2017;69(3):411-420.
Aldosterone Synthase Inhibitors (ASI)
Aldosterone is a key component of RAAS. It is produced in the zona glomerulosa of the adrenal cortex. It is involved in fluid and electrolyte balance and increases sodium and water retention at the distal convoluted tubules in the kidneys. It also causes vasoconstriction and increases fibrosis, all of which contribute to HT. The rate-limiting enzyme responsible for the synthetic pathway from 18-OH corticosterone to aldosterone is aldosterone synthase. Recently, inhibition of ASI has been proposed as a strategy to control aldosterone-dependent HT. Several trials have been carried out targeting this pathway
Selective Inhibition of aldosterone synthase is difficult because it shares 93% sequence similarity with another enzyme that catalyses cortisol synthesis.6 The current attention in this class of drugs is focused on baxdrostat, which shows high selectivity for inhibiting aldosterone synthesis without affecting cortisol levels as compared to the previous ASI agents.7 Baxdrostat binds to the active site of the enzyme, preventing it from catalysing the conversion of corticosterone to aldosterone, thus reducing aldosterone levels and decreasing the RAAS activity. In Phase 1 studies, baxdrostat demonstrated high selectivity for aldosterone synthase inhibition (100:1) compared with cortisol synthesis and reduced plasma aldosterone levels without affecting cortisol levels.
The BrigHTN was a multicenter, randomised placebo-controlled dose-finding trial. It randomised 275 patients with uncontrolled HT who were taking 3 or more antihypertensive drugs at maximally tolerated doses, including a diuretic. Three doses, 0.5 mg, 1 mg and 2 mg were tested.8 After 12 weeks, the trial was stopped by the Data and Safety Monitoring Board (DSMB) for overwhelming superiority. Doses of 2 mg and 1 mg produced a significant reduction in BP. This was accompanied by reduction in aldosterone levels and compensatory rise in renin activity.
Importantly, serum cortisol levels did not change, indicating selective inhibition of aldosterone production. Currently, a new large trial, Bax-HT9 is under way, enrolling patients with uncontrolled HT on 2 drugs or RHT on 3 or more drugs, one of which must be a diuretic in both the arms. It is likely to report in 2025.
Endothelin A/Endothelin B Receptor Antagonists (ETA, ETB)
Endothelin-1 is a vasoconstrictor peptide which is produced in several tissues, particularly in the endothelium of blood vessels. Its action on receptors in smooth muscles causes vasoconstriction, and on endothelial receptors, leads to vasodilatation.10 Endothelin-1 (ET-1) production is increased in HT and endothelial dysfunction. Blocking this pathway has been another approach to treatment of HT. The studies with bosentan and darusentan have shown conflicting results. Endothelin receptor antagonists (ERAs) appear to be more effective in lowrenin conditions.11 Aprocitentan is a dual endothelial A and B receptor blocker. A randomised double-blind placebo-controlled trial, PRECISION, reported in 2022, involved 730 patients with RHT who were randomized to receive either 12.5 mg or 25 mg aprocitentan or placebo.12 At 4 weeks, both doses resulted in a modest SBP and DBP reduction: -3.8/-3.9 mmHg with 12.5 mg and -3.7/4.5 mmHg with 25 mg. However, aprocitentan, resulted in fluid retention in some patients, which could be a concern in patients with HF or renal diseases. Further investigations into the role of this class of drugs are continuing.
Non-Steroidal MRAs
Both spironolactone and eplerenone are effective in reducing BP by blocking the binding of aldosterone to its receptors which are present in several tissues including the kidneys. However, their use is limited in the presence of hyperkalaemia and chronic kidney disease (CKD). Spironolactone also has side effects like gynaecomastia and sexual disorders. Finerenone, a non- steroidal MRA has been shown to possess greater anti-inflammatory and anti-fibrotic properties as compared to spironolactone. It has been shown to be effective in providing renal protection in patients with marked albuminuria and advanced CKD as seen in the FIDELIO-CKD trial in patients with diabetic kidney disease (DKD).13 These results were complemented by the FIGARO-DKD trial which enrolled patients with type-2 diabetes with severe CKD and moderate albuminuria or mild CKD with severely elevated albuminuria.14 In a pooled post-hoc analysis of both these trials, patients with RHT and glomerular filtration rate (GFR) of 25-45 ml/min/1.73m2 and baseline potassium (K) between 4.3 and 5.1, experienced SBP reduction by -7.1 mmHg with finerenone and -1.3 mmHg by placebo (p<0.0001).15 An additional advantage of the drug is the absence of adverse effects of steroids and lesser incidence of hyperkalaemia.
By reducing proinflammatory mediators and fibrosis in the kidney and heart, finerenone may contribute to the management of RHT. Recently a large trial, Fine-ARTS trial was published which explored the role of finerenone in patients with HF with preserved ejection fraction (HFpEF).16 The trial met its combined primary end point of reducing hospitalisation for heart failure (HHF) and death with a significant p value (<0.006). The benefit was driven by reduction in HHF with a modest mortality reduction. Considering that HT is an important contributor to HFpEF, the use of finerenone in HT becomes promising.
Zilbesiran
Angiotensinogen is primarily synthesised by the liver and is the sole precursor of all angiotensin peptides. Interference in its production is another approach towards RAAS and may limit compensatory angiotensin activation associated with angiotensin-converting–enzyme inhibition or angiotensinreceptor blockade. Among the novel drugs being developed for HT is zilbesiran. It is an investigational RNA interference therapeutic agent (siRNA) that binds with high affinity to the hepatic asialoglycoprotein receptor, resulting in specific reduction in hepatic angiotensinogen messenger RNA (mRNA) levels, thereby reducing the production of angiotensinogen.17 Moreover, with hepatocyte-targeted delivery, extrahepatic angiotensinogen effects may be preserved, limiting off target effects in the kidney and other tissues.18 By its unique mechanism of action, it suppresses angiotensin up to 6 months resulting in effective BP control with 2-3 injections a year. In a phase 1 study, KARDIA-1, involving patients with HT, doserelated decreases in both serum angiotensinogen levels and BP after single subcutaneous doses of zilbesiran were observed, that were sustained for up to 24 weeks.19 KARDIA-2 study was presented in April 2024 in which zilbesiran was tested on top of the standard medical care in inadequately controlled HT. It enrolled 672 patients who had elevated BP despite already taking antihypertensive medications. Zilbesiran resulted in statistically significant additional reductions in their 24-hour ambulatory SBP compared with placebo. The incremental reduction in BP as compared to indapamide was 12 mmHg, amlodipine 9.7 mmHg, and olmesartan 4 mmHg. Differences were sustained up to month 6 in the indapamide and amlodipine cohorts. Addition of zilbesiran to any of these drugs did not result in any new serious safety concerns with regard to K, BP or acute kidney injury (AKI). KARDIA-3 is a new ongoing study which will test the efficacy and safety of zilebesiran in patients with hypertension uncontrolled on 2-4 anti-HT drugs with high CV risk or advanced CKD.
Firibastat
Unlike the other drugs targeting the systemic RAAS, this drug is an aminopeptidase inhibitor which acts centrally by lowering the conversion of angiotensin-II to angiotensin III in the brain.20 Reduction in angiotensin III levels in the brain result in lowering of BP. A phase III trial of firibastat, a first-in-class inhibitor of APA in the brain (FRESH) was carried out.21 The trial randomised 514 patients in 11 countries who had SBP 140-180 mmHg despite treatment with at least two or three classes of antihypertensive agents. After 12 weeks of treatment, there was no difference in the active and placebo arms in office BP and AMBP. Because of these results, another larger trial testing the same drug, (REFRESH) trial, was prematurely interrupted and dropped.
Vaccines for HT
Attempts have been made to develop a vaccine for HT. Targets have included angiotensinogen, angiotensin I and II, calcium channels, B1 receptors, and various combinations for multivariant vaccines. So far, they are only in development stages and not ready for any major trials.
Conclusion
Hypertension is the commonest CV disorder and is a significant contributor to CV morbidity and mortality. Despite the availability of several classes of antihypertensive drugs, BP is uncontrolled in a vast majority of patients. The quest for newer antihypertensive agents goes on and several novel drugs are under investigation. Sacubitril/valsartan is a powerful vasodilator and is often effective where the other drugs have not been successful. Aldosterone synthase inhibitors, mRNA interference drugs like zilbeseran, the aminopeptidase A inhibitor firibastat, and the endothelin antagonist aprocitentan are some of the promising drugs which are under clinical trials, but not yet available for clinical use. There is also added interest in the available drugs such as finerenone due to their demonstrable benefits in HT.
The way we practice medicine appears to be poised for major changes. The new therapeutic agents are likely to be more targeted with lesser frequency of administration and minimal side effects to improve compliance. The development of siRNAs, oligonucleotides and monoclonal antibodies to tackle various diseases is progressing at a rapid pace. Admittedly, these therapeutic and diagnostic agents are expensive at present, but with time and greater utilisation, their cost is likely to decrease significantly, increasing their greater utilisation.
Vijay Kumar Chopra. Newer Antihypertensive Drugs. MMJ. 2025, March. Vol 1 (5).
References
- National Family Health Survey -NFHS -5. Available at: https:// mohfw.gov.in/sites/default/files/NFHS-5_Phase-II_0.pdf. Accessed on: 10th December 2024.
- Ruilope LM, Dukat A, Böhm M, et al. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: a randomised, double-blind, placebo-controlled, active comparator study. The Lancet. 2010;375(9722):1255-66.
- Williams B, Cockcroft JR, Kario K, et al. Effects of sacubitril/ valsartan versus olmesartan on central hemodynamics in the elderly with systolic hypertension: the PARAMETER study. Hypertension. 2017;69(3):411-20.
- Jackson AM, Jhund PS, Anand IS, et al. Sacubitril–valsartan as a treatment for apparent resistant hypertension in patients with heart failure and preserved ejection fraction. Eur Heart J 2021;42(36):3741-52.
- Kario K, Rakugi H, Yarimizu D, et al. Twenty four hour blood pressure lowering efficacy of sacubitril/valsartan versus olmesartan in Japanese patients with essential hypertension based on nocturnal blood pressure dipping status: a post hoc analysis of data from a randomized, double blind multicenter study. Am Heart J. 2023;12(8):e027612.
- Amar L, Azizi M, Menard J, et al. Aldosterone synthase inhibition with LCI699: a proof-of-concept study in patients with primary aldosteronism. Hypertension. 2010;56(5):831-8.
- Freeman MW, Bond M, Murphy B, et al. Results from a phase 1, randomized, double-blind, multiple ascending dose study characterizing the pharmacokinetics and demonstrating the safety and selectivity of the aldosterone synthase inhibitor baxdrostat in healthy volunteers. Hypertension Research. 2023;46(1):108-18.
- Freeman MW, Halvorsen YD, Marshall W, et al. Phase 2 trial of baxdrostat for treatment-resistant hypertension. New England Journal of Medicine. 2023;388(5):395-405.
- Perl S, Azizi M, Bakris G, et al. Rationale and design of phase 3 trial for baxdrostat, a novel highly selective aldosterone synthetase inhibitor. Journal of Hypertension. 2024;42(Suppl 1):e259-60.
- Schiffrin EL. Endothelin and endothelin antagonists in hypertension. Journal of hypertension. 1998;16(12):1891-5.
- Chamorro V, Wangensteen R, Sainz J, et al. Protective effects of the angiotensin II type I (ATI) receptor blockade in low-renin deoxycorticosterone acetate (DOCA)-treated spontaneously hypertensive rats. Clinical Science. 2004;106(3):251-9.
- Schlaich MP, Bellet M, Weber MA, et al. Dual endothelin antagonist aprocitentan for resistant hypertension (PRECISION): a multicentre, blinded, randomised, parallel-group, phase 3 trial. The Lancet. 2022;400(10367):1927-37.
- Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383(23):2219-29.
- Pitt B, Filippatos G, Agarwal R, et al. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med. 2021;385(24):2252-63.
- Agarwal R, Filippatos G, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J. 2022;43(6):474-84.
- Solomon SD, McMurray JJ, Vaduganathan M, et al. Finerenone in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2024;391(16):1475-85.
- Morgan ES, Tami Y, Hu K, et al. Antisense inhibition of angiotensinogen with IONIS-AGT-LRx: results of phase 1 and phase 2 studies. Basic to Translational Science. 2021;6(6):485-96.
- Mullick AE, Yeh ST, Graham MJ, et al. Blood pressure lowering and safety improvements with liver angiotensinogen inhibition in models of hypertension and kidney injury. Hypertension. 2017;70(3):566-76.
- Bakris GL, Saxena M, Gupta A, et al. RNA interference with zilebesiran for mild to moderate hypertension: the KARDIA-1 Randomized Clinical Trial. JAMA. 2024;331(9):740-9.
- Marc Y, Gao J, Balavoine F, et al. Central antihypertensive effects of orally active aminopeptidase A inhibitors in spontaneously hypertensive rats. Hypertension. 2012;60(2):411-8.
- Schaffer R, et al. Firbastat fails to improve BP in resistant hypertension: FRESH. Cardiology Today. Available at: https:// www.healio.com/news/cardiology/20221111/firibastat-failsto-improve-bp-in-resistant-hypertension-fresh. Accessed on: 13th December 2024.