

Abstract:
Liver transplant is the only available curative treatment option for unresectable hepatic alveolar echinococcosis. By not receiving the definitive treatment, fatal outcomes may occur in >95% of patients within 10 years. Being a rare disease with even fewer centres indulging in this challenging surgery, literature pertaining to follow-up and management is also scarce. We describe a series of 3 cases of unresectable alveolar echinococcosis who underwent liver transplant along with the challenges involved. One of them underwent retrohepatic caval replacement. They are asymptomatic, have a good quality of life, and are on regular follow-up.
For unresectable hepatic alveolar echinococcosis, liver transplant is a curative option with good long-term results.
Key words: : Liver Transplant, Hepatic Alveolar Echinococcosis.
Introduction
Alveolar echinococcosis (AE) is an accidental zoonotic chronic parasitic disease caused by the ingestion of the eggs of the parasitic cestode Echinococcosis multilocularis (EM). Humans are affected at the larval stage with a primary manifestation in the liver that causes a lethal pathophysiology similar to carcinoma of the liver, if untreated.1,2
According to the World Health Organization (WHO), there are two medically important forms of echinococcosis: (1) cystic echinococcosis (CE) granulosus and (2) alveolar echinococcosis (AE), caused by E. granulosus and E. multilocularis, respectively.1,2 Hepatic echinococcosis is much more seen in AE (99%) vs CE (68%).3 AE is often mistaken for an intra-hepatic invasive tumour-like lesion.
A fatal outcome may occur in >95% of untreated patients within a 10-year period following the diagnosis.4 Diagnosis of AE is based on clinical findings, lesion morphology as determined by imaging techniques, immunodiagnostics, and other laboratory tests.5
Herein, we describe a series of 3 cases of unresectable hepatic alveolar echinococcal infection who underwent liver transplant with curative intent that was performed in the Centre for Liver and Biliary Sciences (CLBS) over the last 3 years.
Case 1
A 27-year-old female from Kyrgyzstan presented with a history of abdominal pain during pregnancy. Imaging showed a cystic lesion in the right lobe of the liver. She underwent an abortion and subsequently a right extended hepatectomy with a diagnosis of alveolar echinococcosis. Albendazole therapy was continued. Unfortunately, upon monitoring she had a recurrence of echinococcosis in the remnant liver.
On examination, she was anaemic and icteric, with a palpable liver with previous laparotomy scar. Laboratory results, apart from alkaline phosphatase (ALP) of 374 IU/L and mild jaundice, were normal. Computed tomography (CT) of the abdomen revealed a residual liver with multiple nodularities along with compression of the portal vein, proper hepatic artery (PHA), and hepatic duct with intrahepatic biliary dilatation.
She underwent a living-related liver transplantation (LRLT) with a modified right lobe graft. Intraoperatively, remnant left lobe liver was enlarged with multiple firm cystic lesions and was adherent to the superior part of the duodenum and pancreas, with notable adhesions in the right subdiaphragmatic space. Recovery was uneventful, and she was discharged on postoperative day (POD) 25. On follow up, she is doing well, with normal graft function and long-term albendazole therapy.
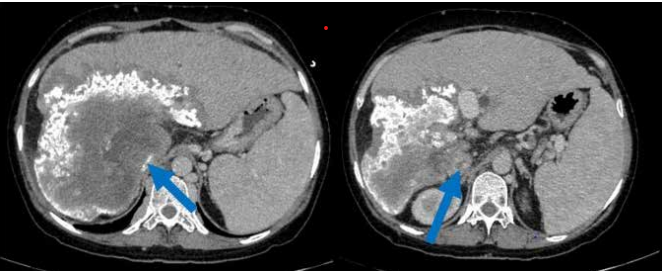
Figure 1: Computed tomography (CT) abdomen (venous phase) shows cirrhotic liver, echinococcal mass encasing the vena cava (blue arrow).
Case 2
A 25-year-old male from Uzbekistan had a history of intermittent abdominal pain for 2 years. Upon investigation in his country, he was found to have multiple liver masses and underwent exploratory laparotomy with a liver mass biopsy. Intraoperative findings noted a hard nodular mass in segment 2 and 4 of the left liver lobe and another lesion in right lobe segment 5, 6, and 8, with multiple small separate lesions. Hard nodular deposits were found near the upper border of the pancreas abutting the aorta and left renal vein posteriorly. Biopsy results reported a benign inflammatory lesion. He was referred to Max Hospital for further evaluation. On clinical examination, the patient was unremarkable. A cross-sectional scan revealed multiple cystic lesions with puckering of the diaphragm and abutting pericardium.
In view of multiple unresectable hydatid lesions, a LRLT was planned. Intraoperatively, there were dense perihepatic
adhesions, multiple hard masses within the liver that were densely adherent to the diaphragm and pericardium, with intense desmoplastic reaction around the mass. He underwent LRLT and received a right lobe graft with no blood transfusion.
Patient had an uneventful postoperative recovery. Patient was able to gradually return to normal diet. Patient was discharged on POD 15 and is doing well, with discontinuation of albendazole after 2 years
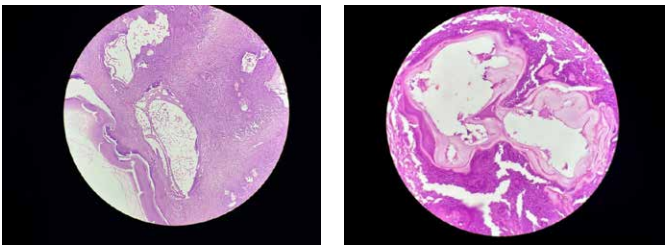
The final histopathology of all the three patients confirmed hydatid disease in the background of cirrhotic liver (as shown in figure 3).
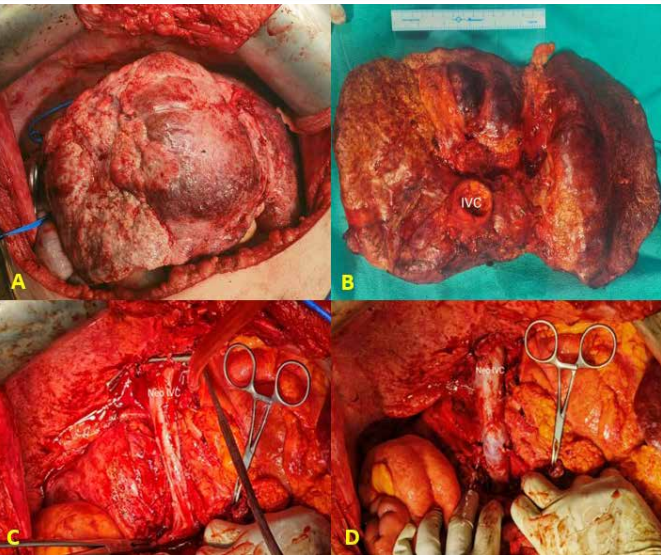
Figure 2: This figure describes intraoperative liver explant and neo-caval creation. (A) shows a macronodular, cirrhotic liver with multiple echinococcal mass. (B) shows posterior aspect of liver explant with en bloc resection of the vena cava. (C) shows status post-neo vena cava creation (clamped). Lastly, (D) shows neo-cava created which is unclamped and full.
Case 3
A 46-year-old female from Uzbekistan, was diagnosed with long standing echinococcosis and was taking albendazole therapy. She complained of intermittent abdominal and pedal oedema along with jaundice, body weakness and abdominal pain. Upon examination, her abdomen was soft. However, her liver and spleen were palpable. Liver function tests (LFTs) were deranged. Imaging revealed a large right-sided alveolar hydatid cyst with involvement of long segment of the inferior vena cava (IVC), encasing the right hepatic vein and draping the left hepatic vein (Figure 1).
The final histopathology of all the three patients confirmed hydatid disease in the background of cirrhotic liver (as shown in figure 3).
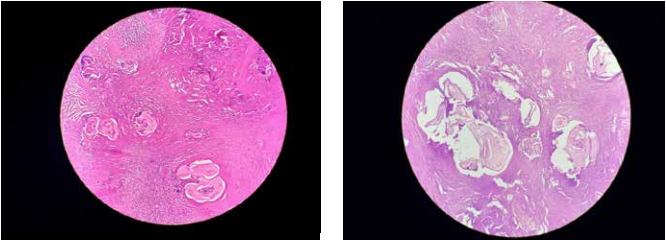
Figure 3: Photomicrograph showing multiple cystic structures with laminated membranes against a necrotic background with occasional preserved bile ducts.
Operative findings:
Intraoperatively, the liver was enlarged, macronodular, and cirrhotic, with a calcified lesion on the surface densely adherent to the retrohepatic cava, which had to be cross-clamped and resected en bloc (Figure 2A and 2B).
A cadaveric graft of the iliac vein was used for venoplasty (Figure 2C and 2D). She underwent LRLT and received a right lobe graft. Reconstruction of IVC, which was encased and infiltrated by the parasitic lesion, was performed using a cryopreserved cadaveric internal iliac artery graft post-endarterectomy.
The liver was explanted along with an en bloc resection of the vena cava (infrahepatic-suprarenal cava and suprahepatic cava) resection (Figure 2B).
The patient had an uneventful recovery, was discharged on POD 20, and is on long-term albendazole therapy along with lifelong oral anticoagulation.
Discussion
Human AE is a potentially fatal, chronically progressive hepatic infestation characterised by a long asymptomatic period, during which an invasive tumour-like lesion develops.6
Hepatic AE is often detected incidentally. According to the FrancEchino registry 2020-2022, 59% of incidental AE cases were discovered during routine imaging for unrelated conditions. Diagnosis is established based on clinical, imaging, and serological results.
The primary screening tests for the diagnosis of AE are Em2 and Em2/3-10 tests, which use EM antigens, whereas the western blot method is used as a secondary test.7 Antibody levels specific to AE gradually decline after surgical treatment and typically become negative within approximately 18 months.8,9
We did not perform these as the lesions in our series of patients were pathognomonic on radiology.
The histopathology revealed irregular cysts with laminated membrane, without a germinal membrane or protoscolices, along with invasion of the liver parenchyma, leading to inflammatory/ granulomatous reactions, extensive peripheral necrosis, and fibrosis.
The optimal treatment for patients having hepatic AE is radical surgery, described as en bloc removal of the lesion with a safe margin (>1 mm), which contrasts with hydatid cyst wherein early lesions have been proven to have therapeutic efficacy. Conversely, at the time of diagnosis, some patient present with an advanced state, making radical surgery unfeasible.6 Option for palliative surgery is not advised. According to R. Mamedov et al., his palliative surgery may technically not be curative as there are areas of extensive involvement and sometimes major vasculature may have invasion.
Liver transplantation (LT) is the treatment option for unresectable hepatic AE. Currently, indications for LT with AE as per WHO are: (1) severe liver insufficiency or recurrent cholangitis as life threatening (2) radical resection is not feasible (3) absence of extra-hepatic diseases7 . Overall mortality rate for post-LT cases is 25%-45%, which is attributed to more advanced disease prior to LT.5
Challenges to this major surgery include a high incidence of vascular involvement, predominantly retrohepatic IVC involvement. Graft procedures are described in subjects with this vascular invasion. Additionally, duct-to-duct anastomosis is often not possible in patients with biliary invasion, necessitating Roux-en-Y hepaticojejunostomy.
Neoadjuvant therapy with albendazole is generally indicated to stabilise the said disease and adjuvant therapy is used against recurrence.4
We treated 3 complicated cases of AE, with one of them requiring an en bloc removal of retrohepatic VC, and its replacement with cadaveric cryopreserved allograft iliac artery. These patients are on regular lifelong follow-up post LT. Immunosuppression is being continued for all three patients. Albendazole was discontinued in one patient after 2 years, while the patient who underwent IVC reconstruction is on prolonged anticoagulation
The Max CLBS team has performed more than 4,500 liver transplants till date. E. multilocularis is relatively common in the Commonwealth of Independent States (CIS) countries, where it is considered endemic.9 The invasive nature of the disease often creates diagnostic dilemma with hepatocellular malignancies. Surgical challenges arise from the infiltrative and adhesive nature of the disease and often needs caval replacement. Post-surgery albendazole is essential, albeit there is debate regarding the duration of such treatment.
Conclusion
For unresectable hepatic AE, liver transplant is a curative option with good long-term results
Aman Chopra, Bappaditya Har, Tejal Bhikubhai Bhoy, Rajesh Dey, Subhash Gupta, Neha Kapoor. Liver
Transplantation in Alveolar Echinococcosis: A Case Series. MMJ. 2025, March. Vol 1 (5).
References
- Craig P. Echinococcus multilocularis. Curr Opin Infect Dis 2003;16:437-444.
- Aydinli B, Pirim I, Polat KY, et al. Association between hepatic alveolarechinococcosis and frequency of human leukocyte antigen class I and II alleles in Turkish patients. Hepatol Res. 2007;37:806-810.
- World Health Organization (WHO), Echinococcosis. 2022 fact sheet. Available at: https://www.who.int/health-topics/ echinococcosis. Accessed on 22nd October 2024.
- Bresson-Hadni S, Koch S, Miguet JP, et al. Indications and results of liver transplantation for Echinococcus alveolar infection: an overview. Langenbecks Arch Surg. 2003;388:231- 238.
- Koch S, Bresson-Hadni S, Miguet JP, et al. Experience of liver transplantation for incurable alveolar echinococcosis: A 45-case European collaborative report. Transplantation 2003;75:856-863.
- Haider HH, Nishida S, Selvaggi G, et al. Alveolar Echinococcosis induced liver failure: salvage by liver transplantation in an otherwise uniformly fatal disease. Clin Transplant. 2008;22:664-667.
- Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev. 2004;17:107-135.
- Biava MF, Dao A, Fortier B. Laboratory diagnosis of cystic hydatic disease. World J Surg. 2001;25:10-14
- Torgerson PR, Keller K, Magnotta M, et al. The global burden of alveolar echinococcosis. PLoS Negl Trop Dis. 2010;4(6):e722.