

Abstract:
Conceptualisation and delivery of oncosurgery services in a new setup comes with its own challenges. However, a clear vision for delivering high - end comprehensive cancer care, supported by a dedicated team, can go a long way in mitigating these challenges. With the rising burden of cancer and scarcity of quality care, a focussed and organ-specific team effort lays the foundation for success.
In this manuscript we describe our journey of performing the initial 100 cases in a new setup, highlighting the challenges faced, and the strategies implemented to mitigate them. Key initial steps, like team building, community outreach programs, and addressing logistical issues, were specifically important and are discussed in detail. We successfully provided surgical treatment across a broad strata of cases, ranging from early-stage to advanced and recurrent cancers, involving multiple organs and primary sites. Our patients included different age groups, ranging from adolescents to geriatric individuals, including cases requiring complex care and multidisciplinary surgical teams.
Key words: Oncosurgery, Comprehensive Cancer Care, Challenges, Milestone.
Introduction
Brief overview of oncosurgery and its importance
The history of treating tumours by surgery dates way back to ancient times when it was the only available modality of cancer treatment. Egyptian writers have described surgical techniques for solid tumours as early as 1600 BC. In the fifth century, Leonidas reported the first surgery for breast cancer— mastectomy. In the 19th and 20th centuries major advances occurred, further refining its role. William Halsted described the technique of radical mastectomy in the late 19th century. Other major contributions include the concept of metastasis by Stephen Paget, an English Surgeon, and the development of the art and science of cancer surgery by Bilroth, Handley and Halsted.1
The significance of surgical oncology lies in its role as the primary treatment modality for many cancers, either alone or in combination with other therapies such as radiation and chemotherapy. Surgery aims to cure the disease, define its stage, or alleviate symptoms, depending on the stage of the cancer and patient situation.
Motivation and vision behind starting the oncosurgery setup
The motivation behind starting the oncosurgery unit was primarily driven by the increasing incidence and projected rise of cancer cases in India, with the true numbers likely much higher than that reported.2 Additionally, a lack of dedicated cancer facilities with the necessary infrastructure and trained personnel further underscored the need for a specialised unit.
Max Super Speciality Hospital is a pioneer in healthcare at every location, with each of its units formally equipped with the latest infrastructure and technologies for oncology care. The vision for this new unit was to provide comprehensive cancer care to patients suffering with this malady.
Summary of the milestone achieved: The first 100 cases
After the inception of the unit in a new setup, within a short span of three months, we successfully performed 100 complex surgical cases with excellent outcomes. These included a wide spectrum of cases ranging from early-stage to advanced and recurrent cancers, involving multiple organ sites and primary tumours. Patients varied in age from adolescents to the elderly, and some required complex care involving multidisciplinary surgical teams. This achievement was made possible through meticulous planning, a strong and focused team, and continuous administrative support. Further description about cases are provided in section 7.
Conceptualisation and Planning
Identifying the need for a new setup in the chosen location
Our aim was to advance the oncology services to the next level in the chosen location. Dwarka, located in South-West Delhi, India, has a population of 1,200,000 as of January 2025, with a population density 21,000 people per square kilometre.3 It is one of the largest sub-cities in Asia. Despite its dense population, oncology centers in this region remain limited, highlighting the necessity for a dedicated oncology unit.
Challenges during the planning phase: Space, funding, regulatory approvals, etc.
Starting services in a greenfield hospital posed several challenges. The foremost challenge was acquiring dedicated spaces for the outpatient department (OPD), inpatient department (IPD) and operation theatres (OTs). Oncosurgeries require a more complex infrastructure compared to general surgical specialties, necessitating significant time and financial investment to reach an optimal level. Advanced equipment like the Hyperthermic Intraperitoneal Chemotherapy System (HIPEC) and robotic system required approvals from hospital authorities before procurement and implementation.
Strategies to overcome these challenges, such as partnerships and resource optimisation
To circumvent the challenges, we optimised available resources and posted cases based on priority and equipment availability. We partnered with existing surgical teams that had already been functional for a few months, allowing us to share instruments and advanced surgical tools, ensuring seamless operations despite infrastructural limitations.
Building the Team and Infrastructure
- Recruitment of a skilled multidisciplinary team (surgeons, anaesthetists, nurses, technicians)
A major requirement for an oncosurgery setup was assembling a skilled, dedicated, and oncology-focused team. Planning for team recruitment began months prior to the unit’s inception to ensure every individual joining the team was outstanding in their work. The surgeons were organ-specific specialists, trained at premier oncology institutes across the country. Anaesthetists had specialised experience in onco-anaesthesia, while nurses and technicians were trained in oncology care to ensure seamless support.
- Setting up state-of-the-art facilities and ensuring adherence to safety standards
Strict quality assurance measures were implemented at every stage, from prehabilitation, and preoperative care to postoperative management. We ensured that the surgical facility met the highest and recommended standards.
- Training and onboarding new team members
New members joining the team underwent supervised training to ensure quality standards. The duration of training varied based on individual background and prior experience.
Initial Challenges
In the initial phase, we encountered several challenges, including:
- Gaining patient trust in a newly established setup
- Establishing community outreach initiatives
- Logistical hurdles like supply chain issues and procedural delays
- Financial constraints and patient affordability
Strategies for Success
Few golden points that paved the way for success included:
- Emphasis on teamwork and communication
- Early adoption of technology and innovative surgical practices
- Continuous medical education and skill development programs for the team
- Building a patient-centric approach with emotional and social support systems
Cutting-Edge Surgical Techniques
We performed complex, high-quality surgeries adhering to International standards including:
- Organ or function preservation surgeries, such as fertilitysparing surgery for young women of reproductive age, sphincter preservation, breast conservation surgery, and limb-salvage procedures
- Minimally invasive surgeries, such as advanced laparoscopic procedures and robot-assisted oncosurgery
- Other advanced techniques
- Video-assisted thoracoscopic surgery (VATS)
- HIPEC for peritoneal surface malignancies
- Secondary cytoreduction
- Complex cancer surgeries involving multi-organ resection
- Oncoplasty and reconstructive surgery
- Image guided procedures, including sentinel node mapping, and vascular assessment at anastomotic sites
- Salvage surgery
Achieving the Milestone
Total number of registered cases in the OPD:
A total of 248 cases were registered in the OPD. The distribution of cases according to Disease Management Groups (DMGs) is depicted in the pie chart (Figure 1).
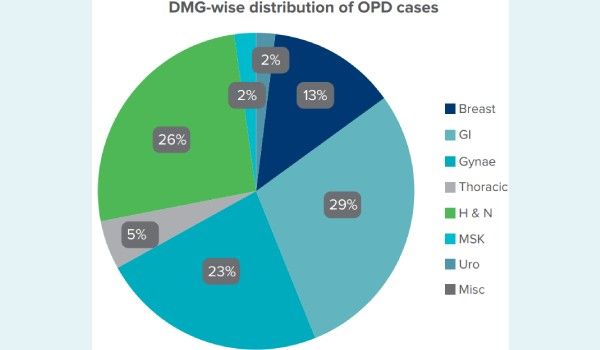
Figure 1: DMG-wise distribution of cases registered in the OPD.
Abbreviations: DMG: disease-management group; GI: gastrointestinal; Gynae: gynaecologic; H & N: head and neck; MSK: musculoskeletal; OPD: outpatient department; Uro: urologic; Misc: miscellaneous.
Key statistics and details of the first 100 cases (types of cases, complexity, outcomes)
Organ of origin: Figure 2 depicts the DMG-wise distribution of operated cases.
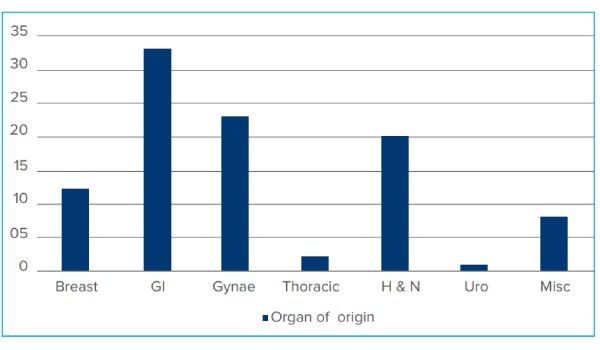
Figure 2: Organ of origin of first 100 operated cases.
Abbreviations: GI: gastrointestinal; Gynae: gynaecologic; H & N: head and neck; MSK: musculoskeletal; Uro: urologic; Misc: miscellaneous.
Patient characteristics:
Median age and range: Median age of operated cases was 52 years, ranging from 13 to 79 years. Nineteen percent of cases were under 40 years of age while 10% were over 65 years.
Sex distribution: The majority of patients were female, comprising 65% of operated cases, while males accounted for 35%.
Surgical techniques and complexity: Minimal access surgery: Twenty six percent of cases were performed using minimally invasive approaches. Their distribution is depicted in the Figure 3.
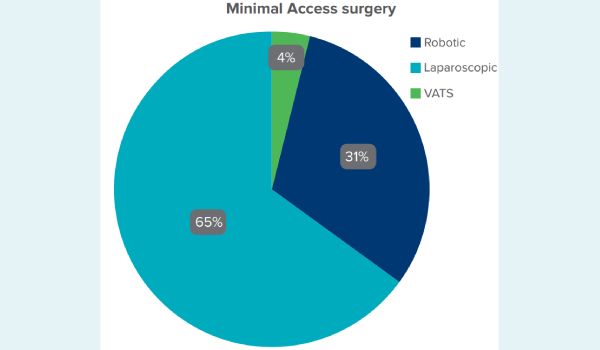
Figure 3: Distribution of different modalities of minimal access surgery
Abbreviation: VATS: Video - Assisted Thoracoscopic Surgery
Of the 26 cases, a laparoscopic approach was utilised in 9 gastrointestinal (GI) and 8 gynaecological procedures, while a robotic approach was used in 8 cases, and VATS was performed in 1 case. Cases performed using the robotic approach included hysterectomy, salpingo-oophorectomy, thymectomy, cholecystectomy, low anterior resection, intersphincteric resection, abdominoperineal resection, and radical antegrade modular pancreatosplenectomy
Cytoreductive surgeries (CRS) and HIPEC for peritoneal surface malignancies: Nine cases underwent CRS, of whom 3 were done along with HIPEC (Figure 4).
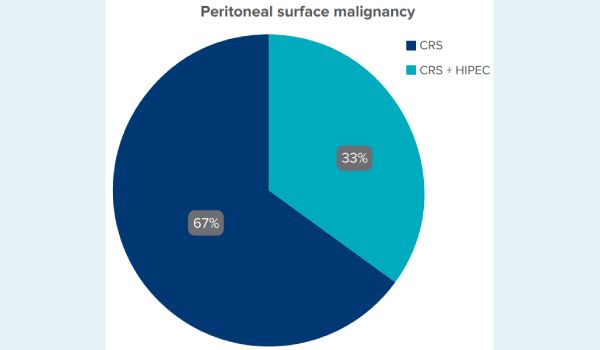
Figure 4: Distribution of procedures for peritoneal surface malignancies.
Abbreviation: CRS: cytoreductive surgery; HIPEC: Hyperthermic Intraperitoneal Chemotherapy.
- Organ or function and fertility preservation: Fertility sparing was performed in 6 cases which included conization for cervical cancer, cystectomies or unilateral oophorectomy for ovarian tumours and hysteroscopic resection for endometrial cancer. Sphincter sparing was done in two cases of rectal cancer whereas breast conservation in 6 cases
- Onco-plastic reconstruction: Ten percent cases underwent reconstructive procedures which included local flaps and free flaps.
- Intraoperative blood transfusion was performed in 10 cases.
- Average length of intensive care unit (ICU) stay was 1 day (range 1-4 days).
Outcomes
- Median length of stay and range: The median length of hospital stay was 5 days (range: 1-14 days).
- Readmissions within the first 30 days: There were no readmissions within the first 30 days after surgery.
- 30-day mortality: There was one mortality within the first 30 days after surgery.
- Clavien-Dindo (CD) grade of complications (major): Major CD complications were observed in three cases.
- Minor cases: Minor cases included biopsies in 25 cases and Human Papilloma Virus (HPV) deoxyribonucleic acid (DNA) sampling for 15 cases.
Lessons Learned
This journey was filled with lessons from each new case. However, the most important ones include:
- Insights gained from overcoming challenges
- Importance of adaptability, leadership, and perseverance
- Reflection on what could have been done differently
Future Directions
With this experience, we aim for the following in near future:
- Expanding the setup, incorporating new techniques and research endeavours
- Setting up a comprehensive cancer centre in next six to twelve months
- Vision for increasing patient access and community impact
Unique Selling Points
- Every cancer center has its unique selling points. Ours include:
- Organ-specific DMGs
- High-end surgical expertise
- Use of advanced and latest techniques–Da Vinci Xi system, image-guided surgeries, ICG, 4k system and 3D laparoscopic system, and lasers
- Precision oncology–organ, function, and fertility preservation
- Multidisciplinary tumour board meetings and personalised cancer treatment
- Pain and palliative care services
- Survivorship program
- Focus on quality-of-life issues beyond cancer care
Conclusion
Setting up a new oncosurgery unit comes with its own challenges, especially given the rising burden of cancer in India. A long-term vision, meticulous planning, coordinated teamwork of organ-specific surgical teams, use of advanced and latest techniques, multidisciplinary case management, and a focus on quality-assured outcomes can play a significant role in establishing a high-end oncosurgery unit.
Sarita Kumari, Shilpi Sharma, Aditi Chaturvedi, Aditi Bansal, Badal Shelke, Jasbir Singh Khanuja, Sanjeev
Kumar. From Challenges to Milestones: Starting an Oncosurgery Unit and Completing 100 Successful
Cases at Max Super Speciality Hospital, Dwarka, Delhi. MMJ. 2025, March. Vol 1 (5).
References
- Lawrence Jr W. History of surgical oncology. InSurgery: Basic Science and Clinical Evidence. 2008 (pp. 1889-1900). New York, NY: Springer New York.
- Sathishkumar K, Chaturvedi M, Das P, et al. Cancer incidence estimates for 2022 & projection for 2025: result from National Cancer Registry Programme, India. Indian J of Med Res. 2022;156(4-5):598-607.
- Dwarka, District South West, Government of India. Demographic data [Internet]. Available at: https://dmsouthwest.delhi.gov.in/ about-district/. Accessed on 16th January 2025.