

Abstract:
Intravenous fluids are arguably the most widely prescribed medications in acute care setting. Like other classes of medications, fluid prescriptions require several considerations—the right indication, the right drug (fluid), the right dose, the right monitoring and the right duration. While appropriate prescription can be life- and organ saving, irrational prescriptions can worsen organ dysfunction and increase mortality. This article reviews the current evidence supporting the rationale prescription of intravenous fluids in acutely ill patients.
Key words: Intravenous Fluids, Electrolyte Balance, Intensive Care Unit (ICU).
Introduction
Intravenous fluids are among the most widely used medications prescribed in the acute care setting. Fluids are prescribed for the resuscitation of patients in circulatory shock, maintenance of fluid and electrolyte balance, replacement of ongoing losses, as diluents for medications, and as flushing solutions. However, not uncommonly, fluids are administered without any clear indication, overlooking their potential harms. Some of the harmful consequences of fluid prescriptions include fluid overload, damage to the endothelial glycocalyx, tissue oedema, organ dysfunction, electrolyte imbalances, metabolic acidosis, and hypothermia.1 In this brief review, we will discuss proven strategies aimed at maximising the benefits and minimising the harms of intravenous fluid prescriptions. These strategies will be discussed in the context of a typical intensive care unit (ICU) patient with septic shock, though they can be extrapolated to other clinical scenarios as well.
Stages of Fluid Therapy
Based on the typical circulatory and metabolic responses observed following an acute insult, four distinct (but dynamic) phases of fluid therapy have been proposed: Resuscitation (or Rescue) Phase, Optimisation Phase, Stabilisation Phase, and Evacuation Phase (acronym R-O-S-E, Figure 1).2 Other authors have named these phases somewhat differently as: Salvage Phase, Optimisation Phase, Stabilisation Phase and De-escalation Phase (acronym S-O-S-D).3
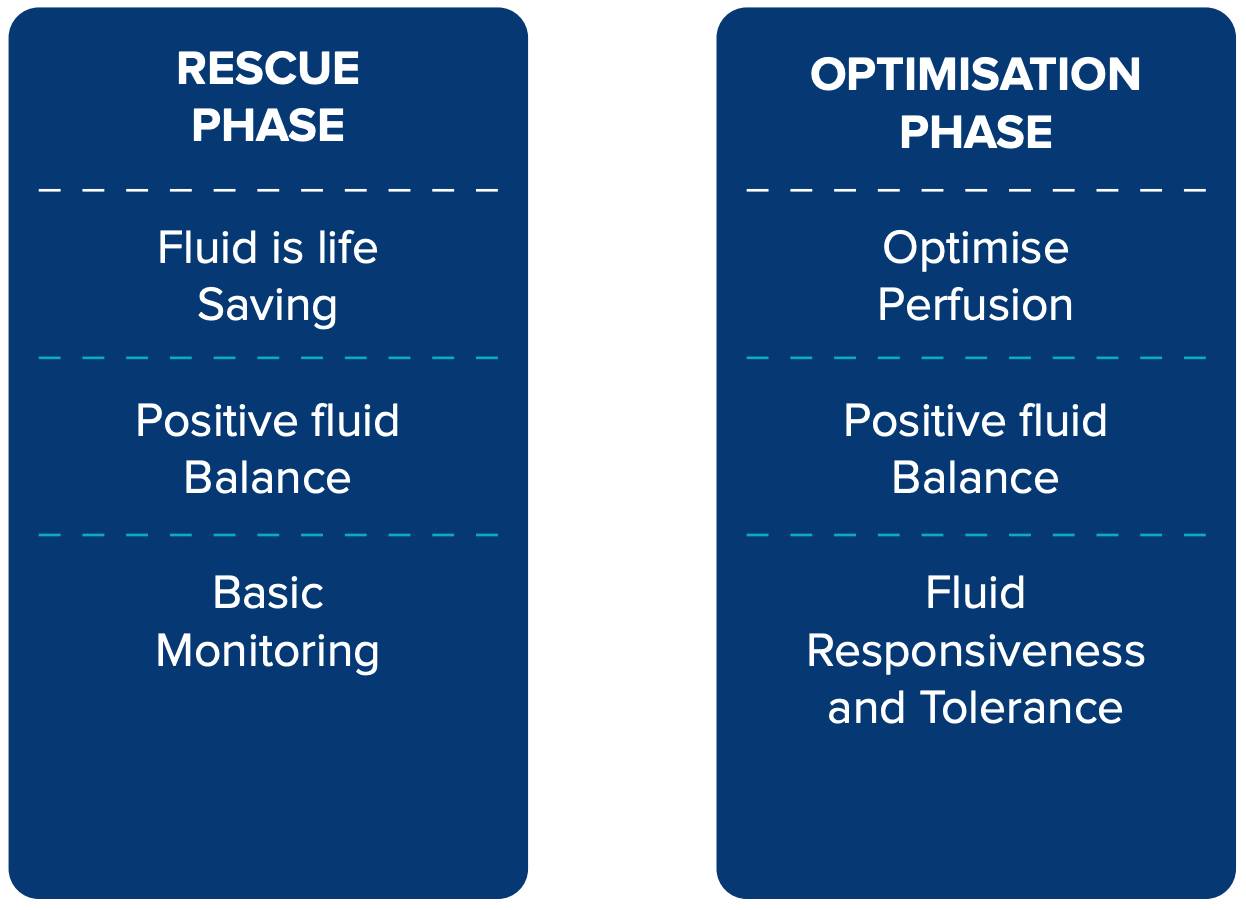
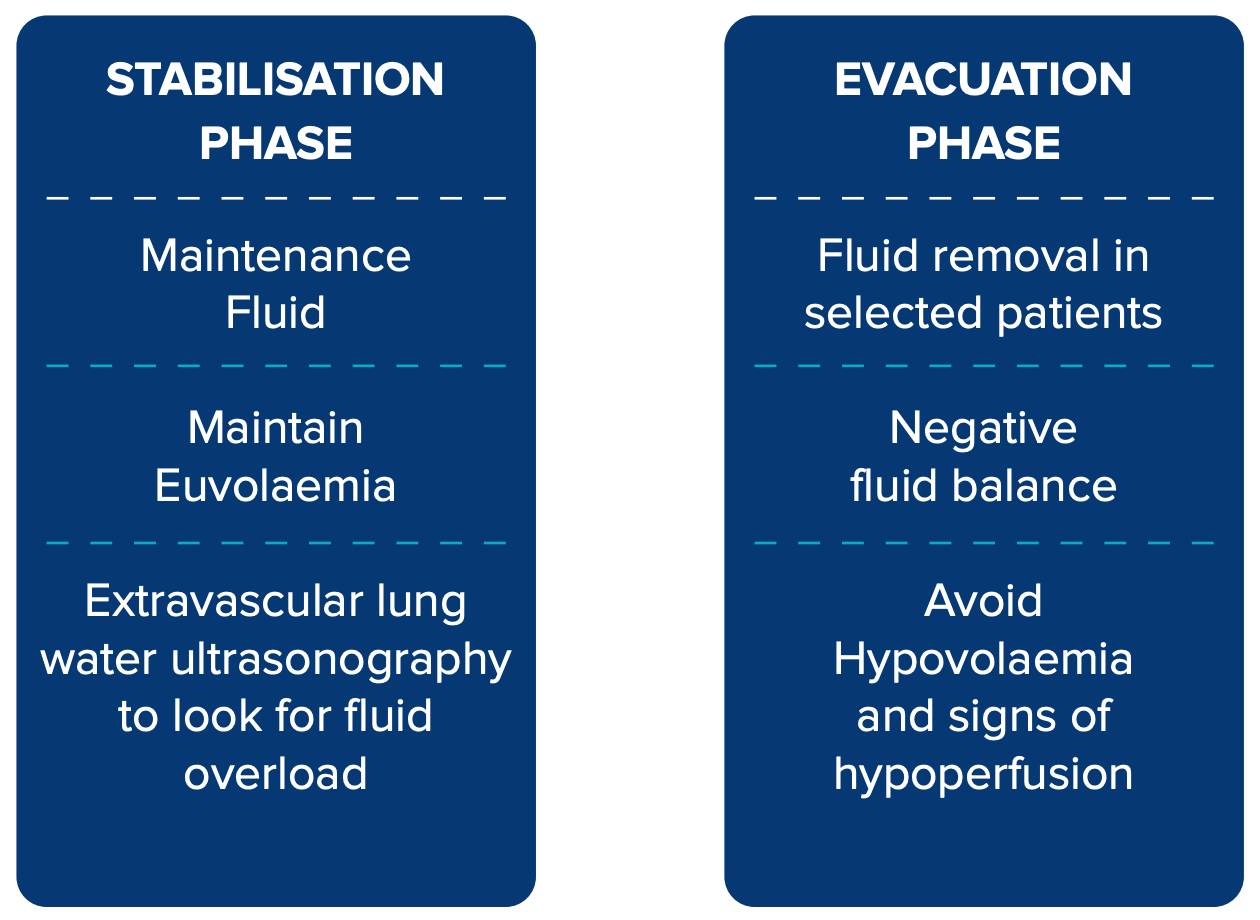
Figure 1: Phases of fluid therapy.
Resuscitation phase
In this phase, also known as rescue or salvage phase, fluid is given as boluses to rapidly correct hypovolaemia, with the goal of achieving minimal cardiac output and blood pressure to sustain life.
- During this phase, patients are monitored clinically using peripheral perfusion markers, blood pressure, heart rate, level of sensorium, lactate etc.
- By the end of this phase (not definitively defined but possibly after initial fluid boluses or within 3-6 hours of the onset of shock), the patient is typically in a positive fluid balance.
Optimisation phase
In this phase, patients are in compensatory shock, either following initial resuscitation or due to their own homeostatic response, and are no longer in an imminent life-threatening state.
- The goal of fluid therapy at this stage is to optimise cardiac output further without worsening reperfusion injury.
- This is achieved by giving small fluid boluses, provided the patient remains fluid-responsive and fluid tolerant.
- This phase requires more sophisticated monitoring, including tests for fluid responsiveness, cardiac output monitoring in selected patients, and careful monitoring for extravascular fluid accumulation by lung ultrasound or extravascular lung water.
- Decision to infuse fluid at this phase also should consider the appropriate clinical context like ongoing volume loss due to diarrhoea or harm of continuing fluid in a patient with pneumonia and severe hypoxaemia.
Stabilisation phase
In this phase, the patient is no longer in circulatory shock or at risk of impending shock, requiring only maintenance fluids to meet the body’s obligatory needs or replacement fluids to correct ongoing volume losses.
- The goal is to keep the patient euvolaemic. Any positive fluid balance can contribute to worsening organ function.
- If all progresses well, the patient should show signs of recovery over the next 2-3 days.
Evacuation phase
Some patients continue to show evidence of capillary leak even during stabilisation phase and develop global increased permeability syndrome (GIPS).2
- GIPS is further aggravated by positive fluid balance in stabilisation phase and a strategy of “late goal directed fluid removal” may be beneficial in such patients.4 The term “de-resuscitation” has been coined to describe this process of fluid removal and is now widely used in the field of intravenous fluid therapy.5
In the subsequent paragraphs, we shall discuss several proven strategies that can be applied in different stages of fluid therapy to minimise harm.
Rescue Phase
Minimise initial resuscitation volume: The Surviving Sepsis Campaign guidelines suggest infusing 30 ml/Kg over 3-hours for every patient with septic shock.6 However, this recommendation is based on limited evidence. A potentially better strategy would be to individualise initial fluid volume based on the clinical response. One way is to follow the original description of intravenous fluid therapy by Sir Thomas Latta ‘‘...having no precedence to guide me I injected ounce after ounce of fluid closely observing the patient.’’7 Based on pharmacokinetic data, the minimum volume of fluid to be administered should be 4 ml/Kg.8
Early initiation of norepinephrine
In patients with vasodilatory or distributive shock, early initiation of vasopressor, especially norepinephrine, has got several beneficial effects:
- Early reversal of life-threatening hypotension
- Reduction in the duration of hypotension9
- Increase in cardiac output10
- Increased mean systemic filling pressure and venous return
- Improved coronary perfusion
- Effect of norepinephrine on the beta-1 receptor
- Potential reduction in cumulative fluid balance11
- Earlier reversal of shock12
Norepinephrine infusion should be initiated if the patient meets any of the following criteria:
- Low diastolic blood pressure (DBP): The aim is to restore coronary perfusion rapidly. In patients with postpartum haemorrhage, troponin rise was observed with DBP less than 50 mmHg.
- Extreme vasodilatation: A very wide pulse pressure reflects extreme vasodilatation. In patients with septic shock, Diastolic Shock Index >2.3 is suggestive of vasodilatation and could be a trigger for starting norepinephrine infusion (Diastolic Shock Index = Heart rate/ Diastolic blood pressure).13,14
- After 1-2 Litres of IV fluid: This approach has been shown to reduce cumulative fluid balance.11
Optimisation Phase
Monitored fluid boluses: Patient should be -carefully accessed for fluid responsiveness and fluid tolerance before administering further fluid bolus. A fluid bolus is expected to improve tissue perfusion by increasing venous return and cardiac output by at least 10%-15%. However, only half of the critically ill patients exhibit this increase in cardiac output following fluid bolus administration.15 In the remaining half, fluid boluses contribute only to fluid overload and worsening organ dysfunction. Several bedside manoeuvres have been developed to increase the preload status of the left side of the heart by utilising heartlung interaction or shifting body fluids from the lower body compartment. These manoeuvres help clinicians identify patients whose cardiac output may improve following an actual fluid bolus.2 These tests of fluid responsiveness can potentially prevent unnecessary fluid bolus administration in fluid-unresponsive patients.
However, identifying fluid responsiveness alone does not ensure that fluid bolus administration will not produce venous congestion. A dynamic assessment of tissue oedema and the patient's capacity to tolerate additional fluids without causing organ-damaging venous congestion is necessary. Fluid tolerance refers to evaluating a patient's ability to handle further fluid administration without worsening venous congestion, tissue oedema, and organ dysfunction.16,17 Studies have shown that fluid intolerance or venous congestion may occur in both fluidresponsive and non-responsive patients.18
Figure 2 provides a schematic diagram to decide about the need for fluid boluses in the optimisation phase
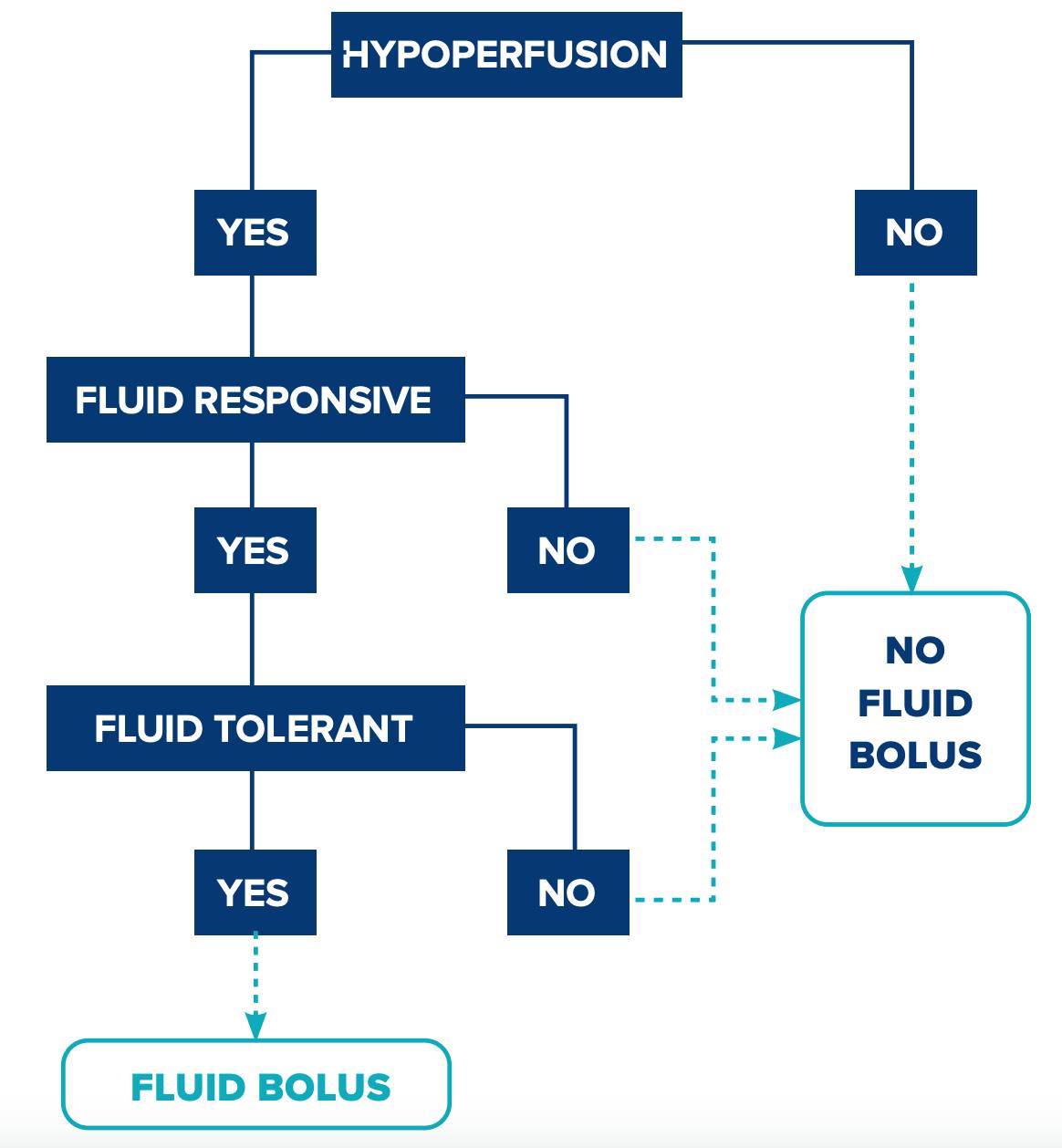
Figure 2: A decision tree for fluid management based on perfusion status, fluid responsiveness, and fluid tolerance.
Hyperoncotic albumin: Unlike hypo-oncotic or iso-oncotic albumin (4%-5%), volume expansion with hyper-oncotic albumin (20%-25%) corresponds with twice the infused volume, both in healthy volunteers and in patients with septic shock.19,20 This volume sparing effect of hyperoncotic albumin is further confirmed by two recent randomised control trials.21,22 Hyperoncotic albumin may be considered a preferred fluid option in the optimisation phase, particularly when crystalloid volume exceeds significantly. However, patient-centered outcomes and cost-benefit ratios of hyperoncotic albumin boluses need to be confirmed in larger studies.
Resuscitation target: Target for resuscitation should be selected carefully for an individual patient. In the ANDROMEDA SHOCK study, patients resuscitated by targeting capillary refill time (CRT) had lower cumulative resuscitation volume than those resuscitated using the same protocol but guided by lactate.23 Kinetics of lactate clearance is much slower compared to CRT.
Stabilisation Phase
Maintenance fluid: In ICU patients, one-third of total fluid intake consists of maintenance fluid, significantly contributing to volume overload.24 Prescription of maintenance fluid should be strictly limited to patients who cannot receive fluids via oral or enteral route. The choice of maintenance fluid can also have an impact on sodium levels and fluid overload. In the TOPMAST study, prescription of isotonic maintenance fluid (Na 154 mmol/L) had a more positive fluid balance and higher rates of clinical fluid overload than those receiving hypotonic maintenance fluid (Na 54 mmol/L).25
Evacuation Phase
De-resuscitation: Patients should be carefully monitored for signs of venous congestion and fluid overload:
- High left or right sided filling pressure(s): Elevated CVP (central venous pressure) is associated with both mortality and acute kidney injury (AKI).26 Echocardiographic measurement of E/e' ratio can be taken as a surrogate of pulmonary artery occlusion pressure.
- Evidence of pulmonary congestion: Examples include extravascular lung water index (EVLWI) or B-profile.27
- Signs of right sided venous congestion: Examples include portal pulsatility index, renal venous impedance index, VEXUS.28,29
Diuresis (or ultrafiltration for patients on renal replacement therapy) should be considered, if venous congestion and volume overload are evident. However, diuresis should not be initiated if there is ongoing resuscitation or evidence of tissue hypoperfusion.
- Simultaneous infusion of 20%-25% albumin can potentiate fluid removal.30
- Low-dose vasopressor infusion can potentially help in redistributing blood volume from interstitial to intravascular compartment.31
- Hypotension is a potential risk during de-resuscitation. The risk of hypotension is significantly higher in patients with evidence of “fluid responsiveness” before initiating diuresis or ultrafiltration. Accessing fluid responsiveness can help predict the safety of fluid removal in a well-perfused patient.32 Simultaneous infusion of 20%-25% albumin may help prevent hypotension.33
- haemodynamic instability (examples include hypotension, rapid fall in cardiac output, prolonged CRT, or worsening lactate levels). De-resuscitation measures should be halted if there is evidence of tissue hypoperfusion and haemodynamic instability
Conclusion
Figure 3 below summarises the current evidence-based strategies to mitigate harm from fluid therapy in a patient with septic shock.
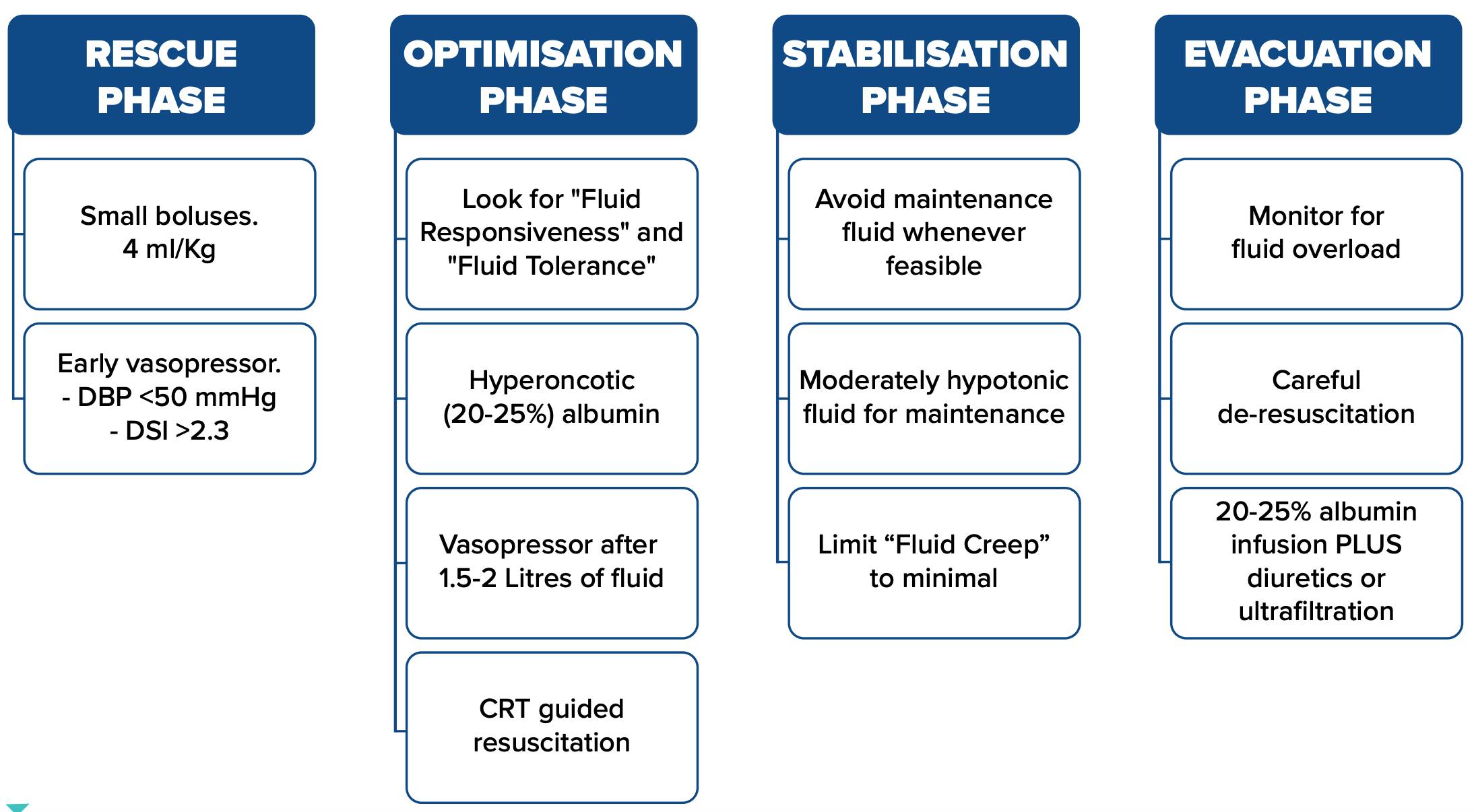
Figure 3: Limiting harm from fluid therapy in septic shock–summarising the evidence. Abbreviations: DBP: diastolic blood pressure; DSI: diastolic shock index; CRT: capillary refill time.
Supradip Ghosh. Less is More: Optimising Fluid Therapy. MMJ. 2025, March. Vol 1 (5).
References
- Van Regenmortel N, Verbrugghe W, Roelant E, et al. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive Care Med. 2018;44(4):409-17.
- Malbrain MLNG, Van Regenmortel N, Saugel B, et al. Principles of fluid management and stewardship in septic shock: it is time to consider the four D's and the four phases of fluid therapy. Ann Intensive Care. 2018;8(1):66.
- Hoste EA, Maitland K, Brudney CS, et al. Four phases of intravenous fluid therapy: a conceptual model. Br J Anaesth. 2014;113:740-7.
- Cordemans C, De Laet I, Van Regenmortel N, et al. Fluid management in critically ill patients: the role of extravascular lung water, abdominal hypertension, capillary leak, and fluid balance. Ann Intensive Care. 2012; 2(Supplement 1): S1.
- Silversides JA, Fitzgerald E, Manickavasagam US, et al. Deresuscitation of Patients with Iatrogenic Fluid Overload Is Associated with Reduced Mortality in Critical Illness. Crit Care Med. 2018; 46:1600-7.
- Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181- 1247.
- Latta TA. Relative to the treatment of cholera by the copious injection of aqueous and saline fluids into the veins. Lancet. 1832; 2:274–7.
- Aya HD, Rhodes A, Chis Ster I, et al. Hemodynamic Effect of Different Doses of Fluids for a Fluid Challenge: A QuasiRandomized Controlled Study. Crit Care Med. 2017;45(2): e161-e168.
- Bai X, Yu W, Ji W, et al. Early versus delayed administration of norepinephrine in patients with septic shock. Crit Care. 2014 ;18(5):532.
- Hamzaoui O, Georger JF, Monnet X, et al. Early administration of norepinephrine increases cardiac preload and cardiac output in septic patients with life-threatening hypotension. Crit Care. 2010;14(4):R142.
- Macdonald SPJ, Keijzers G, Taylor DM, et al. Restricted fluid resuscitation in suspected sepsis associated hypotension (REFRESH): a pilot randomised controlled trial. Intensive Care Med. 2018;44(12):2070-2078.
- Permpikul C, Tongyoo S, Viarasilpa T, et al. Early Use of Norepinephrine in Septic Shock Resuscitation (CENSER). A Randomized Trial. Am J Respir Crit Care Med. 2019 May 1;199(9):1097-1105.
- Karpati PC, Rossignol M, Pirot M, et al. High incidence of myocardial ischemia during postpartum hemorrhage. Anesthesiology. 2004;100(1):30-6.
- Ospina-Tascón GA, Teboul JL, Hernandez G, et al. Diastolic shock index and clinical outcomes in patients with septic shock. Ann Intensive Care. 2020;10(1):41.
- Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008;134(1):172-8.
- Bentzer P, Griesdale DE, Boyd J, et al. Will This Hemodynamically Unstable Patient Respond to a Bolus of Intravenous Fluids? JAMA. 2016;316(12):1298-309.
- Kattan E, Castro R, Miralles-Aguiar F, et al. The emerging concept of fluid tolerance: A position paper. J Crit Care. 2022;71:154070.
- Muñoz F, Born P, Bruna M, et al. Coexistence of a fluid responsive state and venous congestion signals in critically ill patients: a multicenter observational proof-of-concept study. Crit Care. 2024;28(1):52.
- Margarson MP, Soni NC. Changes in serum albumin concentration and volume expanding effects following a bolus of albumin 20% in septic patients. Br J Anaesth. 2004;92(6):821- 6.
- Zdolsek M, Hahn RG. Kinetics of 5% and 20% albumin: A controlled crossover trial in volunteers. Acta Anaesthesiol Scand. 2022 ;66(7):847-858.
- Mårtensson J, Bihari S, Bannard-Smith J, et al. Small volume resuscitation with 20% albumin in intensive care: physiological effects: The SWIPE randomised clinical trial. Intensive Care Med. 2018;44(11):1797-1806.
- Wigmore GJ, Deane AM, Presneill JJ, et al. Twenty percent human albumin solution fluid bolus administration therapy in patients after cardiac surgery-II: a multicentre randomised controlled trial. Intensive Care Med. 2024;50(7):1075-1085.
- Hernández G, Ospina-Tascón GA, Damiani LP, et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients with Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA. 2019;321(7):654-664.
- Van Regenmortel N, Verbrugghe W, Roelant E, et al. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive Care Med. 2018;44(4):409-417.
- Van Regenmortel N, Hendrickx S, Roelant E, et al. 154 compared to 54 mmol per liter of sodium in intravenous maintenance fluid therapy for adult patients undergoing major thoracic surgery (TOPMAST): a single-center randomized controlled double-blind trial. Intensive Care Med. 2019;45(10):1422-1432.
- Chen CY, Zhou Y, Wang P, et al. Elevated central venous pressure is associated with increased mortality and acute kidney injury in critically ill patients: a meta-analysis. Crit Care. 2020;24(1):80.
- De Backer D, Aissaoui N, Cecconi M, et al. How can assessing hemodynamics help to assess volume status? Intensive Care Med. 2022 ;48(10):1482-1494.
- Guinot PG, Bahr PA, Andrei S, et al. Doppler study of portal vein and renal venous velocity predict the appropriate fluid response to diuretic in ICU: a prospective observational echocardiographic evaluation. Crit Care. 2022;26(1):305.
- Rola P, Miralles-Aguiar F, Argaiz E, et al. Clinical applications of the venous excess ultrasound (VExUS) score: conceptual review and case series. Ultrasound J. 2021;13(1):32.
- Martin GS, Moss M, Wheeler AP, et al. A randomized, controlled trial of furosemide with or without albumin in hypoproteinemic patients with acute lung injury. Crit Care Med. 2005;33(8):1681- 7.
- De Backer D, Ostermann M, Monnet X. The nuts and bolts of fluid de-escalation. Intensive Care Med. 2023;49(9):1120-1122.
- Monnet X, Cipriani F, Camous L, et al. The passive leg raising test to guide fluid removal in critically ill patients. Ann Intensive Care. 2016;6(1):46.
- Macedo E, Karl B, Lee E, et al. A randomized trial of albumin infusion to prevent intradialytic hypotension in hospitalized hypoalbuminemic patients. Crit Care. 2021;25(1):18.