

Abstract:
Monoclonal antibodies (mAbs) represent the future of infectious disease management amid rising antimicrobial resistance and emerging pathogens. Evolving from early serum therapies, mAbs now offer targeted and highly specific immune responses through multiple mechanisms, including neutralisation, complement, and cellular cytotoxicity. Several mAbs are approved for infections, including coronavirus disease 2019 (COVID-19), respiratory syncytial virus (RSV), Ebola, human immunodeficiency virus (HIV), and anthrax, with many more in various phases of development. This review explores the structure, types, and clinical applications of mAbs, including newer formats like bi-specific antibodies, mimetics, and antibody-drug conjugates. mAbs also show promise in travel medicine and vaccine development. Their rapid deployment during the COVID-19 pandemic underscores their potential in responding to future public health emergencies
Key words: Monoclonal Antibodies, Antimicrobial Resistance, Passive Immunotherapy, Infectious Diseases, COVID-19, Ebola, RSV, Bi-Specific Antibodies, Antibody Mimetics, Antibody-Drug Conjugates, Vaccine Development, Travel Medicine, Emerging Pathogens.
Historical Perspective1
Antibodies were first used in the late 19th century to treat toxin-producing bacterial infections such as diphtheria and tetanus. Von Behring won the Nobel Prize in medicine for his revolutionary work in diphtheria treatment. This ushered the beginning of the serum therapy era, where animal sera were used against other organisms like Neisseria meningitidis and Group A Streptococcus, though this often resulted in serum sickness. Human sera offered some improvement, but impurities still caused immune complex-mediated fever, rash, and hypotension.
In 1891, Klemperer demonstrated the benefits of serum therapy for Streptococcus pneumoniae when properly administered. However, because the bacterium had multiple serotypes, trials showed that mixing sera targeting various serotypes was better, and this became the standard therapy for pneumonia. However, serum therapy failed during the meningitis outbreaks in the United States of America (USA) and Europe.
The discovery of penicillin by Alexander Fleming in 1928 marked the beginning of the antibiotic era for fighting infections, leading to the abandonment of serum therapy. Nevertheless, sera continued to be used for specific indications, such as snake bites. However, the indiscriminate use of antibiotics opened the Pandora’s box, resulting in the emergence of multi-drug-resistant (MDR) organisms such as Methicillin-Resistant Staphylococcus aureus (MRSA) and Vancomycin-Resistant Enterococcus (VRE). As per the World Health Organisation (WHO) and Centres for Disease Control and Prevention (CDC), antibioticresistant infections are estimated to cause 10 million
deaths annually by 2050, along with a 2%–3.5% reduction in global gross domestic product (GDP). An additional challenge is the emergence of new pathogens such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), along with the re-emergence of others like Ebola. Ebola has a mortality rate exceeding 50%, with no successful treatment options or vaccines. Antibodybased therapies have remained largely experimental, although convalescent sera and monoclonal antibodies (mAbs) were used during the coronavirus disease 2019 (COVID-19) pandemic under emergency use approvals. These recent outbreaks of Ebola and COVID-19, together with the grim scenario of antibiotic resistance, have catalysed renewed interest in mAbs as the next generation of antimicrobial agents. were used during the COVID-19 pandemic under emergency use approvals. These recent outbreaks of Ebola and COVID-19, together with the grim scenario of antibiotic resistance, have catalysed renewed interest in mAbs as the next generation of antimicrobial agents.
Today, antibody treatments are used for diseases like hepatitis B, rabies, respiratory syncytial virus (RSV) infection, tetanus, botulism, vaccinia virus infection, and certain enteroviral infections. These therapies generally involve pooled immunoglobulin (intravenous immunoglobulin, IVIG) from multiple donors, leading to batch-to-batch variability, the need for large quantities due to low specificity, and limited supply dependent on donor availability. The potential of antibodies to treat infections like Plasmodium falciparum, Pseudomonas aeruginosa, Mycobacterium tuberculosis, and Staphylococcus aureus has been under-explored, under-estimated, and under-appreciated.2
In 1975, Cesar Milstein and Georges Köhler developed the first mAbs via fusion of B lymphocytes (B cells) with immortal myeloma cells, an innovation that earned them the Nobel Prize in 1984.
Introduction to Antibodies3,4
Antibodies, or immunoglobulins (Ig), are produced by B cells and play a crucial role in adaptive immunity by neutralising toxins and eliminating pathogens. Ig are found in blood, plasma, and other extracellular fluids (historically called "humors"); hence, their action is referred to as the ‘humoral’ immune response.
An antibody is a Y-shaped molecule, composed of 2 pairs of polypeptide chains: two heavy chains and two light chains. Each chain has a variable region and a constant region. The variable regions of the heavy and light chains together form the antigenbinding site, which determines the antibody specificity. The constant regions are linked by disulfide bonds, providing structural stability to the molecule. The lower part of the Y, known as the fragment crystallisable (Fc) region, consists of constant segments of the heavy chains (Figure 1).
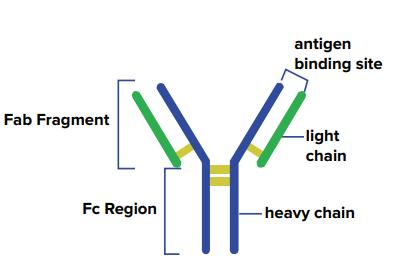
Figure 1: Structure of an antibody.3 The heavy chains (blue), the light chains (green), the disulfide bonds (yellow).
Function of antibodies
-
Neutralising function of antibodies: The antigenbinding site binds to bacterial toxins or viruses, preventing their attachment to and entry into host cells, thereby neutralising the toxins and their harmful effects.
-
Effector functions of antibodies: Effector functions are triggered when the Fc region of an antibody binds to Fc receptors on immune cells after the antibody has attached to an infectious agent or an infected cell. The major effector functions include:
-
Complement activation: Activation of the complement system leads to the lysis of pathogens, a process referred to as complement-dependent cellular cytotoxicity (CDCC).
-
Phagocytosis: Antibodies bound to pathogens enhance their uptake and destruction by phagocytic cells through Fc receptor interactions.
-
ADCC: Antibodies recruit immune cells like macrophages, eosinophils, neutrophils, and natural killer (NK) cells to destroy infected cells via Fc receptor binding.
-
The various mechanisms through which antibodies exert their effects are summarised in Figure 2.
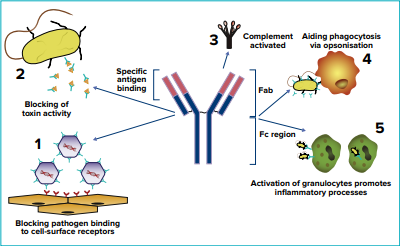
Figure 2: Functions of antibodies.5
Monoclonal Antibodies (mAbs)
Definition: highly purified antibodies produced from a single parent cell, ensuring specificity to one particular target for a disease.
Types of mAbs in clinical use
These antibody types differ in structure and function (Table 1). Over time, the human protein percentage has increased (Table 2).
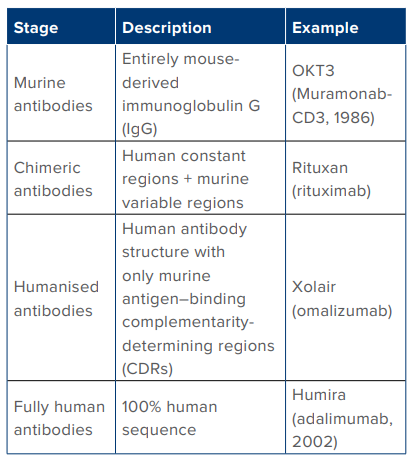
Table 1: Types of monoclonal antibodies in use
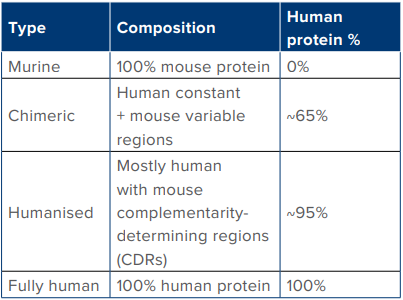
Table 2: Evolution of monoclonal antibodies to fully humanised form.
Nomenclature of mAbs
Pre 2021
Prior to 2021, all mAb names ended with the stem -mab. This naming scheme was replaced in 2021 by the WHO International Nonproprietary Names (INN) nomenclature system, which classifies antibodies based on their structure and target. Examples of pre2021 nomenclature: Altumomab: "-al-" (prefix) + "-tum-" (tumour target) + "-o-" (mouse origin) + "-mab" (suffix) (Table 3)
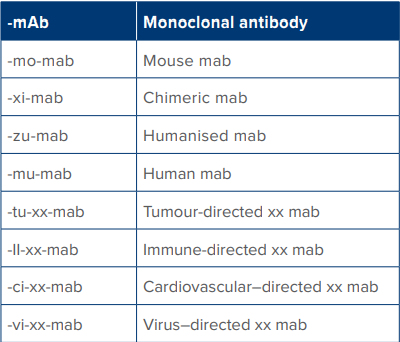
Table 3: Nomenclature of monoclonal antibodies (pre-2021).
Post-20216
The INN nomenclature for mAbs is a combination of a unique prefix, one or more infixes (sub-stems), and a suffix.
-
Prefix: The prefix is random and decided by the manufacturer to ensure distinctiveness.
-
Infix(es): One or more infixes or sub-stems indicate the target and source or purpose.
-
Target (Infix A): Indicates disease or target system.
-
Source/Type (Infix B): Previously indicated the origin (e.g., -o- for mouse) but is largely being phased out to avoid confusion with the new suffix system.
-
Veterinary use: The pre-substem "-vet-" can be used for veterinary products.
-
-
Suffix: A new suffix system has replaced the outdated ‘-mab stem’. As per the 2021 WHO recommendations, the new suffixes for monospecific Ig are as follows:
-
-tug (anti-tumour)
-
-bart (anti-tumour)
-
-mig (multi-specific immunoglobulins)
-
-ment (anti-target for infectious diseases)
-
Thus, under the new system, the suffix indicates the drug's target or function, while the infixes specify the target class (e.g., -ta- for tumour) and where relevant the source of the antibody (e.g., -xi- for chimeric, -zufor humanised).
Example of post-2021 nomenclature for mAbs
Rituximab is a chimeric mAb targeting tumours. Chimeric is denoted by -xi- in the name. If this drug were to be renamed as per INN nomenclature, it would not have -xi-, nor -mab. Also -tu- is no longer used to indicate the target tumour and has been replaced by -ta-. So, ri-tu-xi-mab would be renamed Ri-ta-tug (Ritatug) if it had been named after 2021.
Therapeutic applications of mAbs7
mAbs have both diagnostic as well as therapeutic indications. Diagnostic role includes immunoassays, cancer and disease detection, tissue typing and radio-labelling for imaging purposes. The therapeutic uses are vast and some of these are listed below (Table 4) (Figure 3).
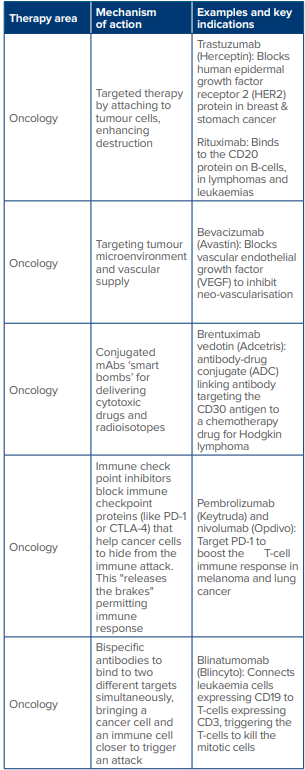
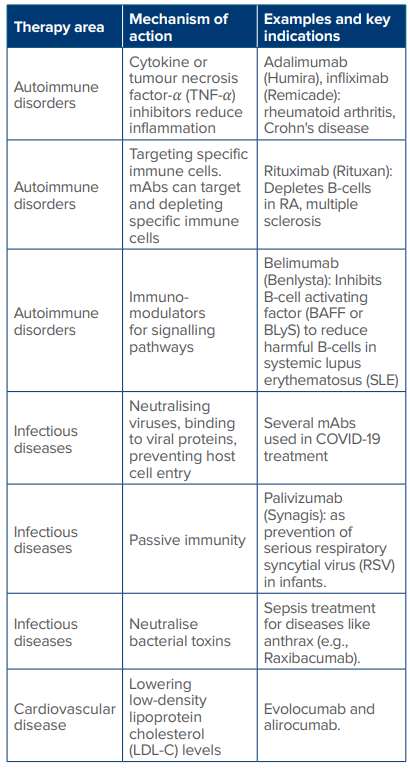
Table 4: Therapeutic applications of monoclonal antibodies (mAbs).
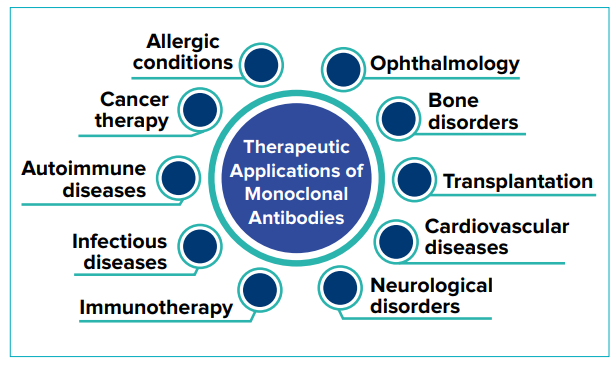
Figure 3: Therapeutic applications of monoclonal antibodies.8
Production of mAbs
Hybridoma technique
In this technique, specific mAbs are produced by fusing antibody-producing B-cells with immortal myeloma cells to create hybridomas, which can continuously secrete large quantities of highly specific identical, highly specific mAbs. The steps in the hybridoma technique include (Figure 4):
-
Step 1 - A mouse is immunised with a specific antigen to elicit an immune response
-
Step 2 - Antibody-producing B cells are harvested from the mouse spleen
-
Step 3 - Harvested B cells are fused with immortal myeloma cells (cancerous B cells) using chemical or electrical techniques
-
Step 4 - Fused cell hybridomas combine B cell’s capacity for specified antibody production with the immortality of myeloma cells
-
Step 5 - Selection of hybridomas and culture to produce massive quantities of a specific mAb
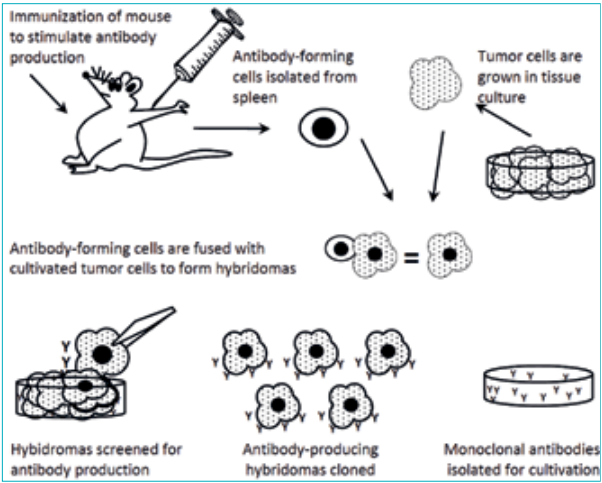
Figure 4: Monoclonal antibody production with hybridoma technology.9
Some of the recent advances in hybridoma technology include the development of technologies for humanised antibody and bispecific antibody production (Figure 5); the use of genetically engineered yeast and mammalian cell lines for large-scale fermentation (up to 5,000 Litres); and improved cell line design and fermentation processes, which have improved specificity and reduced impurities. Additionally, the upscaling production has reduced mAb costs. Currently, mAbs represent the fastest growing segment in the biopharma sector (> 100 billion dollars annually). Moreover, focus has expanded beyond cancer and autoimmune disorders to include infectious diseases.2,11,12
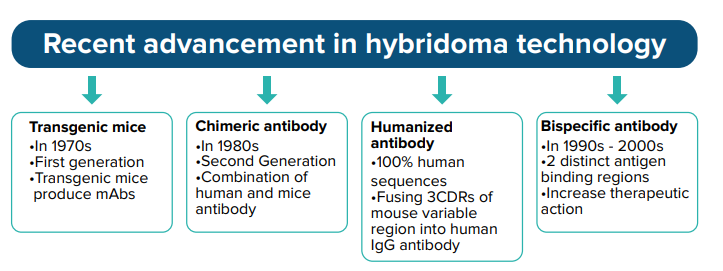
Figure 5: Advances in hybridoma technology.10
Advantages of mAbs over traditional anti-microbial therapy
With the emergence of MDR bacteria, mAbs are going to play a crucial role in the fight against infections in the near future (Table 5).
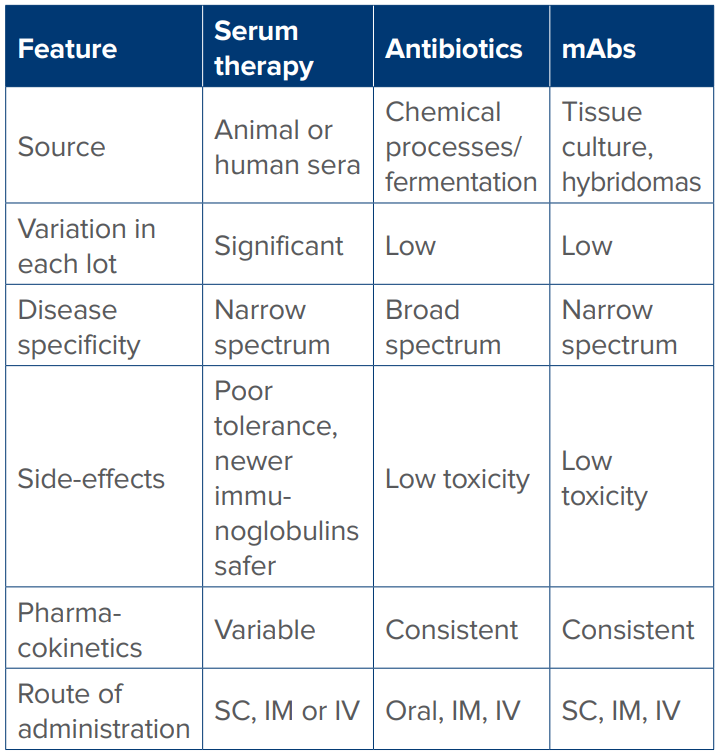
Table 5: Comparison of serum therapy, antibiotics, and monoclonal antibodies (mABs) as anti-microbial therapy.
Abbreviations: SC: Subcutaneous; IM: Intramuscular; IV: Intravenous
Role of mAbs in viral infections (Table 6)
RSV: mAbs including nirsevimab and pallivizumab offer key advantages over vaccines by providing immediate, long-lasting passive immunisation and preventing severe RSV infection in infants and vulnerable young children. Both target the fusion ‘F’ protein of the virus. Nirsevimab, with its extended half-life offers protection for an entire RSV season, whereas pallivizumab requires monthly injections. Notably, plant-based expression platforms have been successfully used for production of recombinant RSV mAbs, which will reduce manufacturing costs compared to traditional mammalian platforms.13
Human immunodeficiency virus (HIV): mAbs can be potentially used in prophylaxis and treatment of MDR HIV in treatment-experienced patients. Ibalizumab has received approval for resistant HIV infection, while broadly neutralising antibodies (bNAbs) such as VRC01 are being tested for long acting pre-exposure prophylaxis (PrEP) and for immune enhancement in long-term treatment. The fact that HIV mutates rapidly remains a challenge.14,15
Rabies: Conventional post-exposure prophylaxis using equine or human rabies immunoglobulin (HRIG) faces limitations due to cost, availability and potential side-effects. mAbs produced by recombinant DNA technology, now offer a safer and more accessible alternative for immediate passive immunity after a potential exposure to the virus following an animal bite. Rabishield and Twinrab are approved for use and are administered by infiltration majorly around the wound site, with the remainder given intramuscularly.16
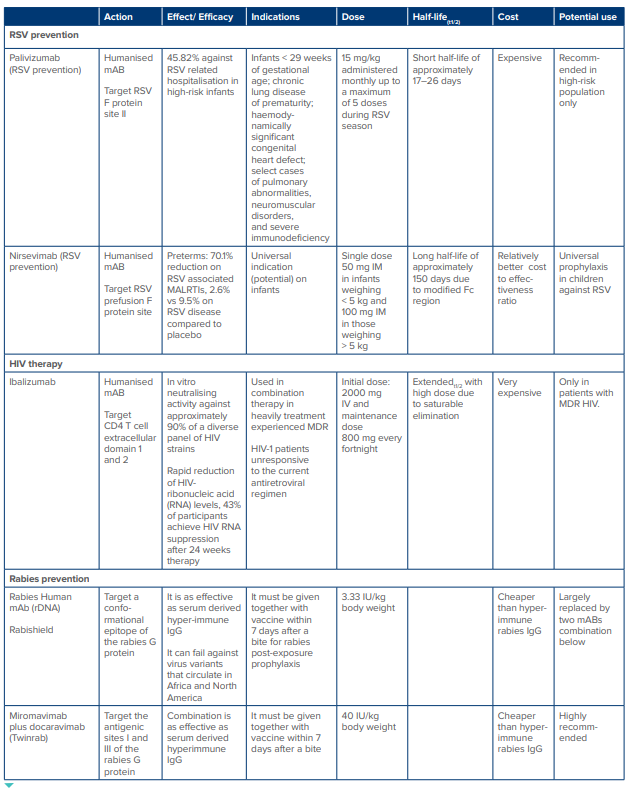
Table 6: Currently approved mABs for RSV, HIV and Rabies virus.17
Abbreviations: mAb: Monoclonal Antibody; RSV: Respiratory Syncytial Virus; MALRTI: Medically Attended Lower Respiratory Tract Infection; IM: Intramuscular; IV: Intravenous; t₁/₂: Half-Life; Fc region: Fragment Crystallisable Region of an Antibody; HIV: Human Immunodeficiency Virus; MDR: Multidrug-Resistant; IgG: Immunoglobulin G; HRIG: Human Rabies Immunoglobulin; rDNA: Recombinant Deoxyribonucleic Acid.
Ebola virus (Table 7): The WHO has approved two mAbs as approved therapies for the treatment of infections caused by the Zaire strain of the Ebola virus. Inmazeb (REGN-EB3) is a cocktail of three mAbs — atoltivimab, maftivimab, and odesivimab — that bind to different, non-overlapping parts of the Ebola virus glycoprotein. Ebanga (mAb114), also known as ansuvimab is a single humanised mAb. These antibodies neutralise the virus by binding to its surface glycoprotein and prevent its entry into host cells. In randomised clinical trials conducted during the 2018–2020 Ebola outbreak in the Democratic Republic of the Congo (PALM Trial), both mAbs demonstrated significant efficacy when administered early in the course of infection. These mAbs are not effective against the Sudan strain of the Ebola virus. Furthermore, they cannot be administered along with the live Ebola vaccine, as it reduces the vaccine’s efficacy.18,19

Table 7: Monoclonal antibodies for Ebola.
COVID-19 infection: mAbs were developed on a warfooting during the COVID-19 pandemic for the treatment of the SARS-CoV-2 infection. Examples include REGENCOV (combination of casirivimab and imdevimab) targeting the virus spike protein, approved by the United States Food and Drug Administration (US FDA) and the European Union (EU) for both treatment and prevention. Other mAbs included bamlanivimab and etesevimab, tixagevimab and cilgavimab, bebtelovimab, and sotrovimab However, the emergence of new SARS-CoV-2 variants posed a major challenge, limiting the continued usefulness of these antibody cocktails. Moreover, multiple studies including a randomized control trial comparing COVID-19 convalescent plasma with mAbs found no difference in efficacy in preventing the need for hospitalisation.20
Role of mAbs in bacterial infections21
With the emergence of MDR pathogens and indiscriminate use of antibiotics, extensive research is underway to explore the use mAbs as anti-microbials. This approach offers greater specificity towards individual targets, unlike broad-spectrum antibiotics, thereby reducing the likelihood of developing antimicrobial resistance. The proposed mechanisms of action of mAbs against bacteria include the following (Figure 6):
-
Neutralisation of bacterial toxins – e.g., bezlotoxumab for Clostridium difficile
-
Inhibition of bacterial adhesion to host cells – e.g., mAbs targeting the Type III secretion system (TTSS) of Pseudomonas aeruginosa
-
Interference with bacterial communication system (quorum sensing) – by blocking quorum sensing (QS) molecules, thereby reducing bacterial virulence
-
Opsono-phagocytosis – by functioning as opsonins, to mark pathogens for enhanced destruction by macrophages and neutrophils
-
Complement-dependent cytotoxicity – by activating the complement cascade
-
Disruption of biofilm – by binding to the scaffolding matrix proteins within the biofilm
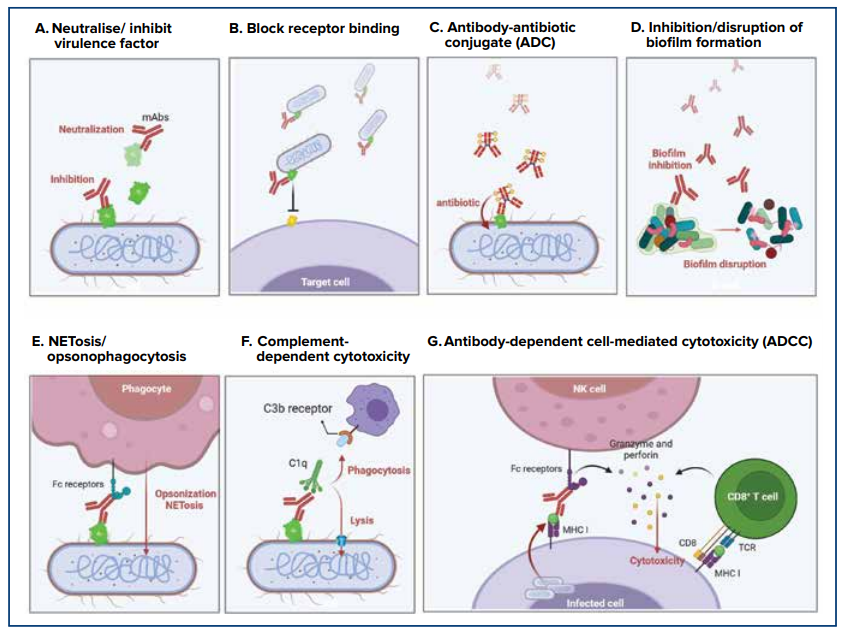
Figure 6: Mechanisms of monoclonal antibodies against bacterial infections.21
Abbreviation: NET: Neutrophil Extracellular Trap.
US FDA-approved antibacterial mAbs18,19
To date, only three antibacterial mAbs had received FDA approval, as follows:
-
Bezlotoxumab (Zinplava®): For adults at high risk of recurrent of Clostridium difficile infection. It works by binding to and neutralising the C. difficile toxin B.
-
Raxibacumab (Abthrax®): For the treatment and prophylaxis of inhalational anthrax caused by Bacillus anthracis. It works by neutralising the protective antigen (PA) component of the anthrax toxin.
-
Obiltoxaximab (Anthim®): For inhalational anthrax. Similar to raxibacumab, it also targets and neutralises the PA component of the anthrax toxin.
Challenges in development of anti-bacterial mAbs:
-
Pathogen diversity: Unlike viruses, bacteria possess hundreds of potential surface antigens and multiple serotypes. Consequently, a single mAb may not provide broad protection, necessitating the development of antibody cocktails targeting multiple epitopes.
-
Target accessibility: A potential target may be masked by the polysaccharide capsule, making it difficult for mAb to bind.
-
Clinical trial failures: Many candidate mAbs have failed in human trials after being found useful in animal models. Moreover, co-administration with antibiotics during studies can confound results.
-
Cost and market size: The research and development of mAbs is very expensive, and the relatively small market size can limit commercial viability.
-
Dependence on rapid diagnostics: As mAbs are highly specific, effective treatment may depend on rapid and accurate diagnosis of the infective pathogen.
The key viral and bacterial targets currently under investigation for mAb development are summarised in Table 8.
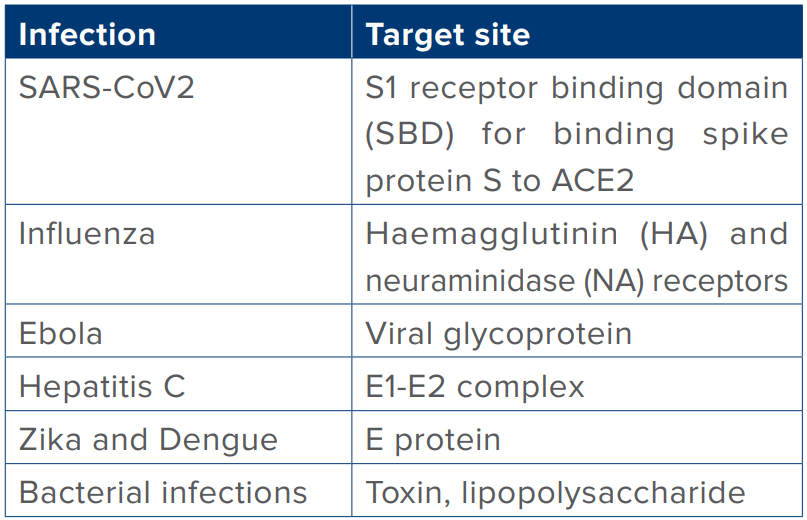
Table 8: Targets for monoclonal antibodies (mAbs) against infectious diseases.
Abbreviations: SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; SBD: Spike Binding Domain; ACE2: Angiotensin-Converting Enzyme 2; HA: Haemagglutinin; NA: Neuraminidase; E: Envelope; E1-E2: Envelope Glycoprotein Complex.
Side-effects of mAbs
When evaluating mAb therapies, it is important to recognise that each mAb is a unique protein, and treatment involves administering a significant quantity of protein through IV, intramuscular, or subcutaneous routes. While mAbs generally have an excellent safety profile in both randomised controlled trials (RCTs) and observational studies, some have been linked to adverse events, which may be related to the specific characteristics of individual formulations. Side effects can include infusion-related reactions, fever, nausea, rash, diarrhoea, and hypotension. For instance, the combination of tixagevimab and cilgavimab was associated with a higher incidence of thromboembolic events compared with other mAbs, while the combination of casirivimab and imdevimab, and bamlanivimab alone, have shown a higher incidence of ischaemic heart disease events. Bevacizumab (Avastin), which targets a protein called vascular endothelial growth factor (VEGF), can cause hypertension, bleeding, thrombotic events, and kidney damage. Similarly, cetuximab (Erbitux), which targets the epidermal growth factor receptor (EGFR), may cause severe skin rashes in some people as EGFR is also present in normal skin cells.
Application of mAbs in travel medicine22
mAbs may be used in travel medicine in the following scenarios in the future:
-
Pre-travel prophylaxis: Passive immunisation using mAbs could prevent diseases such as malaria
-
Post-exposure prophylaxis: mAbs can prevent disease onset after exposure, as already demonstrated in rabies management.
-
Treatment of travel-acquired infections: mAbs may be developed for infections like dengue fever and yellow fever.
Hypothetically, mAbs may offer advantages in certain situations over standard vaccines and prophylaxis methods. For example, using mAbs to prevent Plasmodium falciparum malaria could involve a single injectable dose administered before departure, providing protection without significant side effects, compared to daily or weekly oral anti-malarial prophylaxis. Other examples include single-dose mAb prophylaxis for hepatitis A or yellow fever in immunocompromised travellers who may not be able to produce a sufficient antibody response or where live attenuated vaccines, such as the yellow fever vaccine is contraindicated.
mAbs have also shown promise in treating diseases with high mortality, such as Ebola and yellow fever, and research is ongoing for diseases like rabies and dengue fever.
Emerging mAbs against infectious diseases
Nipah virus: A human clinical trial to test the safety and efficacy of a novel monoclonal antibody, MBP1F5, is expected to begin in India and Bangladesh soon. Nipah virus has a high mortality rate (45%–75%), and currently lacks an approved vaccine.23,24
Dengue: Phase II clinical trials are underway for AV-1, an investigational human mAb developed by AbViro (USA), to mitigate clinical symptoms when administered before or after dengue infection.25
Influenza: mAbs in clinical development for influenza are aimed at treating active infections. Due to the annual variation in circulating strains, most mAbs under development target the highly conserved stem region of the hemagglutinin (HA) protein.
Malaria: Based on promising preclinical results from two mouse models of Plasmodium falciparum infection, the mAb CIS43LS is being developed as a long-acting immune prophylactic against malaria.
Next generation antibodies26
The different formats and types of next-generation antibodies are illustrated in Figure 7.

Figure 7: Next generation antibodies.26
Single-chain variable fragment (scFv) antibodies
mAbs have limitations in treating diseases because of their relatively large molecular size. To address this, smaller scFv recombinant antibodies have been developed. They consist of the variable heavy (VH) and variable light (VL) chains connected by a flexible poly-linker peptide (15–20 amino acids). The bacterial expression system, particularly Escherichia coli, is commonly used for scFv production. The size of scFvs (27 kDa) is roughly one-fifth that of a complete antibody, allowing easier penetration into tumours and accessibility to cryptic epitopes. Moreover, scFvs are cleared more easily from non-target healthy tissues causing lesser side-effects
An scFv is thus a recombinant antibody format composed of a single polypeptide chain that retains the antigen-binding properties inherent in the intact antibody, while offering advantages in size, penetration, and manufacturability.
Bispecific antibodies
mAbs have two arms that each recognises the same target antigen. Bispecific antibodies (bsAbs) have two unique binding domains simultaneously binding to two different antigens, offering an improved therapeutic approach. Early bsAbs were created by chemically combining two mAbs or fusing together two hybridoma cell lines, resulting in ‘quadroma’ cell lines. Recently, genetic engineering advancements have led to the development of more than 50 recombinant bsAbs. Removab (catumaxomab) and Blincyto (blinatumomab) were amongst the first clinically approved bsAbs, used for treating malignant ascites intraperitoneally and for relapsed or refractory B-cell acute lymphoblastic leukaemia (ALL) respectively.
Antibody biosimilars
Antibody biosimilars are biologic drugs that closely resemble approved therapeutic mAbs (reference or originator mAbs) in structure, function, and efficacy. These have to replicate the safety, efficacy, and quality of the original mAbs, they are not identical to the originator molecule. Several biosimilars for including infliximab, rituximab, trastuzumab, and bevacizumab have been approved. These are more affordable although efficacy maybe lower.
Antibody mimetics
Antibody mimetics, or "synthetic antibodies," are designed to mimic the functions of natural antibodies by replicating their antigen-binding segments, minus the Fc region and associated issues. These are more stable and cost-effective.
Antibody drug conjugates (ADCs)
ADCs combine the specificity of mAbs with the potent cytotoxic effects of small-molecule drugs. ADCs selectively deliver powerful anticancer agents directly to tumour cells, minimis ing the systemic toxicity that typically accompanies chemotherapy eg. adotrastuzumab emtansine (Kadcyla) for human epidermal growth factor receptor 2 (HER2) positive breast cancer. ADCs can be used in combination with other oncology treatments to enhance overall anti-tumour effects.
mAbs as vaccines27
Although vaccines remain the most effective preventive measure against infections, effective vaccines have not yet been developed for pathogens such as HIV, RSV, Hepatitis C, and Ebola virus. For a vaccine to be effective, it must elicit a robust and durable antibody response. Identifying antibodies capable of effectively neutralising a pathogen is a key step in hastening vaccine development.
Pathogen-neutralising mAbs are used to identify antigenic structures on the pathogen’s surface. These antigen-antibody complexes are then analysed to select antigenic structures suitable for vaccine design (Figure 8).
The concept of reverse vaccinology 2.0, also known as antibody-based vaccinology, aims to overcome the limitations of traditional vaccine development methods by creating novel vaccines through the use of structural information derived from mAb-antigen complexes. The process starts with single-cell cultures of plasma or memory B cells derived from convalescent patients or vaccinated donors. These cultures are screened to identify mAbs with neutralising activity against the target pathogen. The recombinant mAbs are then used to identify the antigen and analyse the three-dimensional (3D) structure of the antigen-mAb complex. This structural data is crucial for designing and optimizing stabilized antigens for next-generation vaccine development.
Roadmap for mAb use in infection outbreaks
Humanity has faced at least seven major viral outbreaks in the 21st century — SARS-CoV, Middle East respiratory syndrome coronavirus (MERS-CoV), influenza A (H1N1), Zika virus, Ebola virus, SARS-CoV-2, and monkey pox (Mpox) — and must brace ourselves for further outbreaks. The war-paced development and deployment of mAbs for COVID-19 pandemic stands out as a scientific success story. This accomplishment saved countless lives and established a blueprint for contingency planning in future infectious disease emergencies. To further enhance mAb effectiveness, they could be combined with small-molecule antiviral drugs, which may lower viral loads and minimise the selection of mutant strains. Given the importance of early intervention, widespread use of mAbs will require the establishment of dedicated infusion centres and physician education, so that mAb therapy can be promptly administered to high-risk individuals during future outbreaks.
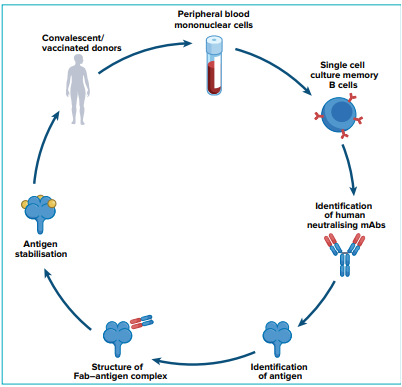
Figure 8: Schematic representation of reverse vaccinology 2.0.27
Conclusion
mAbs have evolved from experimental immunotherapies to essential tools in infectious disease management. Their precision, adaptability, and safety make them promising alternatives to conventional antimicrobials, particularly in an era of rising MDR. Recent advances — including bispecific antibodies, antibody–drug conjugates, and mimetics — have expanded their clinical utility beyond oncology to encompass viral, bacterial, and parasitic infections. The rapid development of mAbs during the COVID-19 pandemic demonstrated their scalability and global relevance. Future priorities include cost-effective production, improved delivery systems, and equitable access to ensure mAbs become integral components of modern antimicrobial therapy.
Sandeep Budhiraja, Monica Mahajan, Arnav Chauhan. From Bench to Bedside: Monoclonal Antibodies as Next-Generation Antimicrobials. MMJ. 2025, December. Vol 2 (4)
References
- Hey A. History and practice: Antibodies in infectious diseases. Microbiol Spectr. 2015;3(2):AID-0026-2014.
- Grace PS, Gunn BM, Lu LL. Engineering the supernatural: monoclonal antibodies for challenging infectious diseases. Curr Opin Biotechnol. 2022;78:102818
- Afaneh C, Aull MJ, Kapur S, Leeser DB. Induction Therapy in Renal Transplant Recipients. In: Kapur S, editors. Immunosuppression – Role in Health and Diseases. InTech; 2012. p. 357–84.
- Pantaleo G, Correia B, Fenwick C, et al. Antibodies to combat viral infections: development strategies and process. Nat Rev Drug Discov. 2022;21(9):685–705.
- Leo O, Cunningham A, Stern PL. Vaccine immunology. Perspectives in Vaccinology. 2011;1(1):25–59.
- World Health Organization. New INN nomenclature scheme for monoclonal antibodies. INN working doc. 22.542. Geneva: World Health Organization; 2022.
- Castelli MS, McGonigle P, Hornby PJ. The pharmacology and therapeutic applications of monoclonal antibodies. Pharmacol Res Perspect. 2019;7(6):e00535.
- Kothari M, Wanjari A, Acharya S, et al. A Comprehensive Review of Monoclonal Antibodies in Modern Medicine: Tracing the Evolution of a Revolutionary Therapeutic Approach. Cureus 2024;16(6):e61983.
- Sarcan ET, Özer Y. Monoclonal Antibodies and Immuno-PET Imaging: An Overview. FABAD J Pharm Sci . 2023;48(1):165–82.
- Mitra, S., Tomar, P.C. Hybridoma technology; advancements, clinical significance, and future aspects. J Genet Eng Biotechnol. 2021;19:159.
- Whaley KJ, Zeitlin L. Emerging antibody-based products for infectious diseases: planning for metric ton manufacturing. Hum Vaccin Immunother. 2021;17(8):2497–505
- Hariharan M, Nithya R. Review on monoclonal antibodies – manufacturing aspects, tactics, and future prospects. Int J Green Pharm. 2022;16(2):143–4.
- Pisuttinusart N, Rattanapisit K, Srisaowakarn C, et al. Neutralizing activity of anti-respiratory syncytial virus monoclonal antibody produced in Nicotiana benthamiana. Hum Vaccin Immunother. 2024;20(1):2327142.
- Chahine EB, Durham SH. Ibalizumab: The First Monoclonal Antibody for the Treatment of HIV-1 Infection. Ann Pharmacother. 2021;55(2):230–9.
- Sofia S, Guimaraes K, Thorpe R, et al. International nonproprietary names for monoclonal antibodies: an evolving nomenclature system. MAbs. 2022;14(1):e2075078.
- Cunningham CK, McFarland EJ, Morrison RL, C, et al. IMPAACT P1112 team. Safety, Tolerability, and Pharmacokinetics of the Broadly Neutralizing Human Immunodeficiency Virus (HIV)-1 Monoclonal Antibody VRC01 in HIV-Exposed Newborn Infants. J Infect Dis. 2020;222(4):628–36.
- Wu M, Peng X, Xu W, et al. Development of Human Monoclonal Antibodies With Broad Reactivity for Rabies Postexposure Prophylaxis. J Med Virol. 2024;96(11):e70068.
- Esposito S, Amirthalingam G, Bassetti M, et al. Monoclonal antibodies for prophylaxis and therapy of respiratory syncytial virus, SARS-CoV-2, HIV, rabies and bacterial infections: an update. Front Immunol. 2023;14:1162342.
- Shcherbakov DN, Isaeva AA, Mustaev EA. Treatment of Ebola Virus Disease: From Serotherapy to the Use of Monoclonal Antibodies. Antibodies. 2025;14(1):22.
- PALM Consortium. Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N Engl J Med 2019;381:255–60.
- Casadevall A, Focosi D. Lessons from the use of monoclonal antibodies to SARS-CoV-2 spike protein during the COVID-19 pandemic. Annu Rev Med. 2024;75:235–250.
- Chen HC, Pan YL, Chen Y, et al. Monoclonal Antibodies as a Therapeutic Strategy against Multidrug-Resistant Bacterial Infections in a Post-COVID-19 Era. Life (Basel). 2024;14(2):246.
- Hanna K, de Jong P, Grobusch PM. Monoclonal antibody applications in travel medicine. Trop Dis Travel Med Vaccines. 2023;9(1):15.
- Rodrigue V, Gravagna K, Yao J, et al. Current progress towards prevention of Nipah and Hendra disease in humans: A scoping review of vaccine and monoclonal antibody candidates being evaluated in clinical trials. Trop Med Int Health. 2024;29(5):354–64
- Prasad R. Nipah monoclonal antibody trials may begin in India in 2025. The Hindu [Internet]. 2024 Feb 2. Available at: https://www.thehindu.com/news/national/nipah-monoclonalantibody-trials-may-begin-in-india-in-2025/article68396911. ece. Accessed on: 6th August 2025.
- Adhikari S, Bhusal S, Hossain M S, et al. Assessment and management of dengue. BMJ. 2025;388:e082639.
- Singh R, Chandley P, Rohatgi S. Recent advances in the development of monoclonal antibodies and next-generation antibodies. ImmunoHorizons. 2023;7(4):886–97.
- Pantaleo G, Correia B, Fenwick C. et al. Antibodies to combat viral infections: development strategies and progress. Nat Rev Drug Discov. 2022;21(9):676–96.