

Abstract:
Methamphetamine is a highly addictive psychostimulant drug derived from amphetamine. It can produce euphoria and stimulant effects like those caused by other stimulants such as cocaine. This case report describes a 22-year-old female who was brought to the hospital emergency department with agitation, tachycardia, hyperthermia, altered mental status, profuse perspiration, and vomiting. The symptoms observed in cases of polydrug toxicity fall into multiple toxidromes, making it a diagnostic dilemma. In this case, the patient was diagnosed with methamphetamine and cocaine toxicity and developed acute liver and kidney injury. She required haemodialysis with specialised filters and prolonged intensive care unit (ICU) stay, but eventually recovered to full strength. This case emphasises the importance of early extracorporeal therapy for multi-organ support and multi-disciplinary approach involving various specialties along with the critical care team, to enhance recovery in toxicity cases.
Key words: Polydrug, Toxicity, Extracorporeal.
Introduction
Substance abuse is a deeply entrenched and multifaceted health issue that causes hundreds of fatal and nonfatal intoxications worldwide. Drug-related deaths most often occur due to polydrug toxicity, typically involving combinations of illicit opioids, other illicit drugs, and benzodiazepines consumed for recreational purposes, which together cause or contribute to the fatal outcomes.1 Toxicological analysis plays a crucial role in identifying the real cause of intoxication, making the implementation of up-to-date good practices essential in toxicology laboratories.2 Accordingly, effective toxicological screening and confirmatory analytical methods should be focused to detect and quantify multiple drug classes within a single analytical protocol.3 In managing such cases, it is crucial to consider both the individual and combined toxic effects of drugs to devise an appropriate treatment plan.
This case report details the complex clinical management of multi-organ dysfunction resulting from polydrug toxicity in a 22-year-old female.
A 22-year-old female resident of Delhi attending an international music concert in Mumbai, presented to the emergency care centre of the concert with complaints of vomiting, profuse sweating, and altered mental status. Immediate intravenous (IV) access was obtained, and the patient was administered antiemetics and IV fluids before being transferred to the emergency department of Nanavati Max Super Speciality Hospital, Mumbai, Maharashtra.
On arrival at the emergency department, the patient was agitated and disoriented. Her vital signs were as follows: pulse rate 180 beats per minute (bpm), blood pressure 100/50 mmHg, oxygen saturation on room air 93% (indicating hypoxia), and temperature 102°F. Pupils were bilaterally 3 mm and sluggishly reacting to light. Her Glasgow Coma Scale (GCS) score was E2V3M5. In view of the poor GCS and continuous vomiting, the patient was immediately intubated for airway protection. As the patient was in altered sensorium and unaccompanied by family, with only friends present at the concert, no reliable past medical history or exact course of the events leading up to her symptoms could be obtained
Patient was shifted to the intensive care unit (ICU), where routine investigations and a urine toxicology screen were performed. The differential diagnosis considered included suicidal poisoning, recreational drug abuse, central nervous system (CNS) stroke, encephalitis, and postictal state.
The Day 1 laboratory investigations revealed: haemoglobin 11.7 g/dL, platelet count 1,67,000/µL, prothrombin time (PT)/international normalised ratio (INR) 14 sec/ 1.3, serum glutamic-oxaloacetic transaminase (SGOT) 120 U/L, serum glutamic-pyruvic transaminase (SGPT) 53 U/L, serum creatinine 2.1 mg/dL, creatine phosphokinase (CPK) 9,082 U/L, and serum ammonia 159 mg/L.
The patient was managed with IV fluids and prophylactic anti-epileptic medication. In view of deranged liver function tests (LFTs), N-acetylcysteine (NAC) infusion was started. Vasopressor support was administered to maintain adequate mean arterial pressure (MAP). Empirical antibiotics (ceftriaxone and doxycycline) were started in view of fever, hypotension and the possibility of atypical infection. Magnetic resonance imaging (MRI) brain was performed, which was essentially normal.
The urine toxicology screen, received the following morning, tested positive for amphetamines, methamphetamine and cannabinoids. Based on the clinical picture and laboratory findings, a diagnosis of serotonin syndrome was established.
The patient fulfilled Hunter’s criteria for serotonin toxicity, which include the presence of spontaneous clonus, inducible clonus with agitation or diaphoresis, ocular clonus with agitation or diaphoresis, tremor and hyperreflexia, or hypertonia with a temperature above 38°C (100.4°F) and ocular or inducible clonus.
The Day 2 investigations indicated worsening multiorgan dysfunction: haemoglobin 13.4 g/dL, platelet count 53,000/µL, PT/INR 47 sec/4.5, SGOT 15,414 U/L, SGPT 8, 312 U/L, serum creatinine 2.8 mg/dL, CPK 19,648 U/L, lactate dehydrogenase (LDH) 11,067 U/L, and ferritin 6,331 µg/L.
The patient developed oliguria with progressive renal and hepatic impairment, necessitating initiation of continuous renal replacement therapy (CRRT).
Given the markedly elevated liver enzymes and evidence of systemic inflammation, haemoperfusion using specialised HA 330 filter was performed on Day 3 and Day 6. The HA 330 extracorporeal haemoperfusion device, containing neutral macroporous resin, is proven to specifically adsorb medium- to large-sized inflammatory mediators, including cytokines such as Interleukin (IL)-1, IL-6, IL-8, and tumour necrosis factor-alpha (TNF-α), thereby reducing the cytokine burden. The serial laboratory are parameters summarised in Table 1.
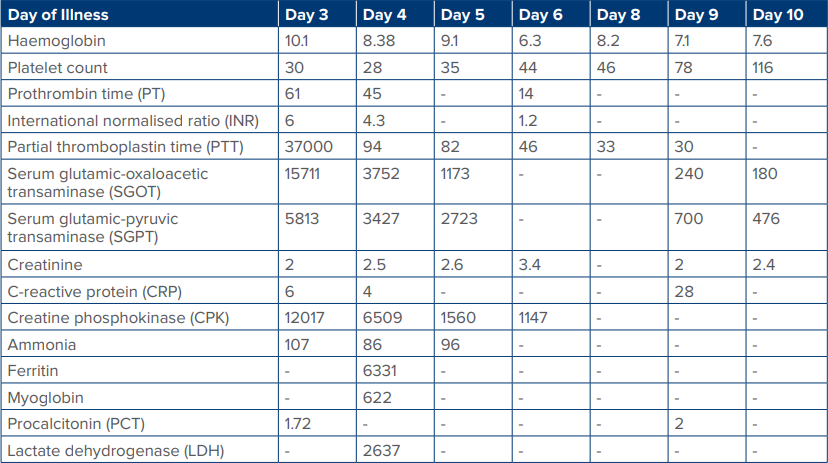
Table 1: Laboratory reports from Day 3 to Day 10
The patient required multiple blood and blood product transfusions during the course of the illness.
From Day 5, sedation holidays were initiated. The patient remained drowsy but was able to obey commands and move all limbs.
On Day 6, the patient developed hypotension with low-grade fever. Pan cultures were sent, and antibiotics were escalated to meropenem and teicoplanin. On the same day, a second HA 330 filter was used. With continued CRRT, the patient’s liver and kidney functions showed gradual improvement, along with haemodynamic stabilisation. Urine culture grew E. faecium, which was vancomycin-resistant but linezolid-sensitive. The antibiotic therapy was then modified accordingly.
On Day 9, furosemide trial was given during ongoing CRRT, to which she responded well, allowing gradual weaning off CRRT. Once haemodynamically stable and with improving laboratory parameters, she was initiated on spontaneous breathing trials and successfully extubated on Day 11.
There was gradual improvement in liver enzymes and creatinine over the next 10 days. The patient was discharged on Day 20 with oral linezolid and supportive medications.
Discussion
Methamphetamine is a highly addictive psychostimulant drug chemically related to amphetamine. It produces intense euphoria and stimulant effects similar to those of cocaine. Owing to its ease of synthesis from inexpensive and readily available chemicals, methamphetamine abuse has become widespread across the world.
The global use of methamphetamine and amphetamine has increased rapidly in recent years. The high accumulation of methamphetamine, a potent stimulant drug, in multiple body organs is likely to contribute to the medical complications associated with methamphetamine abuse.6
In the CNS, amphetamines act by blocking presynaptic reuptake of catecholamines, resulting in hyperstimulation at selected postsynaptic receptors. Their indirect sympathomimetic effects arise from blockade of presynaptic vesicular storage and inhibition of cytoplasmic destruction of catecholamines by inhibition of mitochondrial monoamine oxidase.4,5 Methamphetamine is absorbed readily from the gastrointestinal tract, airway, nasopharynx, muscle, placenta, and vagina. Peak plasma levels are observed approximately 30 minutes after IV or intramuscular routes and within 2–3 hours after oral ingestion. Rapid tissue redistribution occurs, with steadystate cerebrospinal fluid concentrations reaching about 80% of plasma levels. Metabolism occurs primarily in the liver via conjugation pathways involving glucuronide and glycine, followed by urinary excretion of metabolites.
Immediate supportive care is essential and includes airway protection, oxygenation and ventilatory support, and appropriate monitoring. Electrocardiographic (ECG) monitoring and prompt treatment of arrythmias are crucial. Rhabdomyolysis, causing acute kidney injury (AKI) is a common complication and warrants appropriate medical treatment and early initiation of dialysis, if required.
Use of extracorporeal filters and CRRT for liver and kidney injury should be considered early, as they help to maintain electrolyte and hemodynamic balance.
During prolonged hospitalisation and extracorporeal therapy, common hospital-acquired infections should not be missed, and antibiotic therapy should be guided by the hospital antibiogram.
Conclusion
Drug overdose cases present significant therapeutic challenges, as specific antidotes are unavailable for most substances and many drugs undergo complex, multi-pathway metabolism. Management should prioritise rapid stabilisation of airway, breathing and circulation. Timely initiation of therapies affecting drug pharmacodynamics and adequate multi-organ support is key to the treatment of acute intoxication and crucial to improving patient outcomes.
Prachi Kulkarni Biswas, Akanksha Bathija, Abdul Samad Ansari. Polydrug Toxicity: Diagnostic Complexity and Critical Care Strategies. MMJ. 2025, December. Vol 2 (4)
DOI: XXXX
References
- Al Khouri I, Iannaccone B, Fulajtarova M. Trends in Substance Use Among Young People in the EU: A Secondary Analysis of Available Data. Addictology/Adiktologie. 2024;Oct 1(4)
- Zaami S, Busardò FP, Pichini S, et al. The value of toxicological and forensic analyses in the global challenge to health risks caused by new psychoactive substances. Eur Rev Med Pharmacol Sci. 2019;23(14):6008–10.
- Mannocchi G, Di Trana A, Tini A, et al. Development and validation of fast UHPLC-MS/MS screening method for 87 NPS and 32 other drugs of abuse in hair and nails: application to real cases. Anal Bioanal Chem. 2020 ;412(21):5125–45.
- Onuk S, Akin AK, Sari A, et al. The Clinical and Laboratory Efficacy of HA 330 Treatment Combined with Continuous Renal Replacement Therapy in Septic Shock Patients: A Case Series. Blood Purif. 2023;52(2):140–7.
- Kiyatkin EA, Sharma HS. Acute methamphetamine intoxication: brain hyperthermia, blood–brain barrier, brain edema, and morphological cell abnormalities. Int Rev Neurobiol. 2009;88:65–100.
- Volkow ND, Fowler JS, Wang GJ, et al. Distribution and pharmacokinetics of methamphetamine in the human body: clinical implications. PloS one. 2010;5(12):e15269.